I’m working on a post about the role of serotonin in the development and maintenance of anorexia, but it is taking me some time as I want to include a sufficient amount of background information. So, in the meantime, I’m going to blog about a short paper that was brought to my attention by Sarah. As you might have guessed by the title, the paper’s author, Casper Schoemaker, wanted to do some fact-checking on Naomi Wolf’s first book, titled The Beauty Myth. A quick glance at the Amazon ratings reveals that a lot of people like it, and many find it shocking and “eye-opening”. Now, I’ll admit: I haven’t read it, and I don’t plan to. (I don’t read books like this.) But I have come across blatantly wrong statistics on eating disorders from people citing her work.
(Books are not peer-reviewed. The main thing you need to get a book published is to convince the publisher that people will buy it. There’s no guarantee that the claims in a particular book are correct. A lot of times they are not. See Kevin Trudeau, though not everyone lies on purpose.)
If you are wondering who cares? I mean, lots of people get things wrong all the time. And that’s true. But, Wolf is a public figure, her statistics are heavily cited in the media, and the media has a huge impact on the public understanding of eating disorders, and even on clinicians’ attitudes toward patients with EDs. She is not helping the feminist cause nor the eating disorder awareness campaigns by fudging facts.
In her first book The Beauty Myth (Wolf, 1990), the American feminist writer Naomi Wolf asserted that the second feminist wave had not been very successful. In 1990, according to Wolf, women were underpaid, and not judged by the quality of their work, but by their looks. Most well educated women suffered from the eating disorders anorexia and bulimia nervosa, and were forced to end their education. The few women that did not diet put all their money in cosmetic surgery. And the purported cause of all this was the “Beauty Myth.”
Thanks to her debut book, Wolf obtained instantaneous fame all over the world. She traveled, gave lectures, took part in discussions, and appeared on television. Her book was a best seller. In the public debate the anorexia statistics in her chapter “Hunger” were frequently talked about. The eating disorder figures were dramatically high: according to Wolf (1990), 20% of American female students suffered from anorexia and 60% from bulimia. Only small minority had no eating disorder! Her mortality figure—150,000 deaths from anorexia each year in the U.S.—caught the most attention in the media…….
In 1994, professor in philosophy Christina Hoff Sommers—not an eating disorder expert—responded in her book Who Stole Feminism? (Sommers, 1994). She tracked down the mortality figure to the source. Wolf had cited a book by Brumberg, who had referred to a newsletter of the American Anorexia and Bulimia Association (AABA). Brumberg misquoted this newsletter, however: The AABA had referred to 150,000 sufferers (not fatalities) from anorexia nervosa.
So anyway, Wolf corrected herself in later edition of the book. But, was that all? Schoemaker wanted to investigate all the other statistics that Wolf cited (in the newest edition of the book) and compared them with findings in peer-reviewed literature.
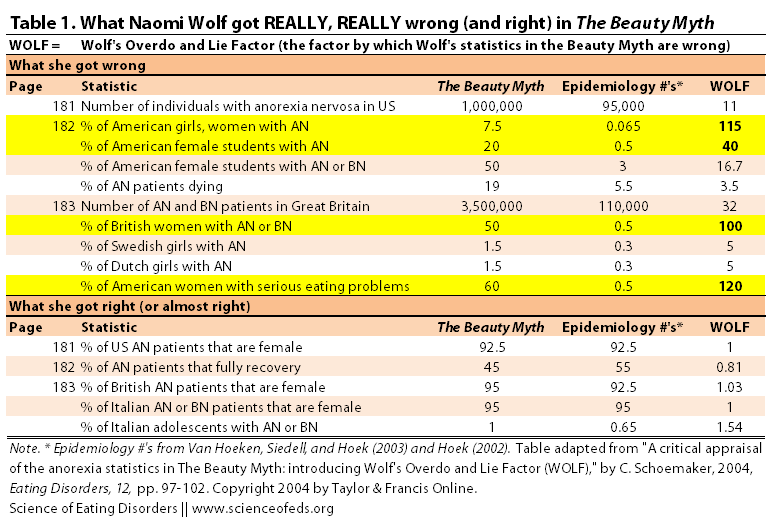
Schoemaker relied on statistics from epidemiological reviews (Hoek, 2002 and Van Hoeken et al., 2003). To illustrate Wolf’s absurd statistics, Schoemaker calculated the factor by which Wolf was wrong, called WOLF (Wolf’s Overdo and Lie Factor). An example: taking Wolf’s original 150,000 annual deaths due to AN, and dividing it by the real number (around .56% of AN patients die a year, which is about 525), you get 286.
Naomi’s original statistics was almost 300 times higher than the real number.
Below is my adapted version of the table from Schoemaker’s paper. I lifted the most outrageous WOLF numbers as well as the statistics that Naomi Wolf got right. There’s only one statistics Wolf underestimates: the number of anorexia patients that fully recover (WOLF = 0.81).
Of course, one can argue that the data in Hoek’s and Van Hoeken’s review papers are not very accurate. They might not be. I haven’t checked, for example, the criteria used to assess whether someone is recovered or not (these vary a lot, there’s no agreed upon definition of recovery). Nonetheless, two reviews of many epidemiological studies to date, published in peer-reviewed journals, are likely to have statistics as good as we can get. And given just how wrong Naomi Wolf was in some of the statistics she cites, I doubt a few percent fluctuation either way in the “epidemiological #’s” would make much difference.
Schoemaker:
The mean WOLF for all 23 anorexia statistics was 8.28. This is after the correction Wolf mentioned in her letter to the editor of Time [about the annual mortality rate]… In summary: On average, an anorexia statistic in any edition of the The Beauty Myth should be divided by eight to get near the real statistic.
In the discussion, Schoemaker makes a few salient points, but the main one is that Wolf is not helping anyone by overdoing the numbers or calling it an “epidemic”. It is not an epidemic, but that doesn’t mean we shouldn’t care about it: “anorexia nervosa is a very serious health problem. Not because of the “epidemic” numbers of patients, however, but because of the devastating effects on the few individuals who develop anorexia.”
Exactly. Clinicians and scientists shouldn’t, and hopefully don’t, start caring about diseases and mental disorders when they reach epidemic proportions. There are lots of health problems that are much rarer than anorexia nervosa that get proper research and medical attention. As they should, because the impact on the patient, their family and society as a whole, is huge. Patients shouldn’t be turned away because their problems are so rare, it is just not worth, from a health economics perspective, to spend money researching the causes and cures, and treating them. Things hopefully don’t work that way. We don’t need to (I hope) exaggerate statistics in a misguided attempt to raise awareness.
I love the snarky ending:
I suggest the experts enter the public debate more often. For that purpose, the WOLF seems to be an easy and useful tool to quantify the exaggerations in the media. Its acronym refers to a writer that should never be trusted with anorexia statistics again.
References
Schoemaker, C. (2004). A critical appraisal of the anorexia statistics in The Beauty Myth: introducing Wolf’s Overdo and Lie Factor (WOLF). Eating Disorders, 12 (2), 97-102 PMID: 16864310
The other problem with exaggerating the stats about a disease to draw attention to it, is that it can leads to those people who really have the disease going without recognition and treatment because they’re lumped together with all the milder cases & people who don’t have it at all.
Seriously. Someone said on an ED blog that anorexics and bulimics simply act on the thoughts of every American woman. Sure, every American woman wants to cry over eating one grape?
Exactly.
Great post Tetyana!
Because of the thrust from well-meaning Feminists, the public, politicians and medical professionals are receiving very unhelpful, mixed messages about the causes of Anorexia Nervosa (AN).
Although we don’t know the precise cause of AN, there is sufficient evidence that it has a strong biological basis and that it affects only a select few in our society. And by ‘select’ [few], I mean people with a particular, inherent vulnerability. This vulnerability seems to relate to temperament, personality characteristics and the presence of autistic traits.
There is absolutely NO epidemic of AN, and the incidence hasn’t increased significantly over the last 30 years, despite huge changes in our culture.
As a consequence of the axiomatic assumption, pedalled by feminists theorists and activists such as Naomi Wolf, that AN is caused by our toxic culture, this very serious illness is often dumbed down and policy makers turn to efforts to change culture rather than to improve treatments, or make treatments and associated funding more widely available.
This has always been my biggest gripe about the whole relationship between body image and EDs. My gripe is not based upon the fact that I had non-fat-phobic AN, but the fact so many people assume that the body image concerns that do exist in AN (when present) come from popular culture/media. This really dumbs down the seriousness of AN as a true illness – and leads to erroneous assumptions that AN can be prevented (or treated) by changing culture – when there is no evidence to support this hypothesis. People with AN need intensive treatment that focuses on helping them to regain lost weight, continue to nourish themselves properly. They usually also need help with anxiety and obsessionality – and channelling their traits down different paths. Many people with AN have co-morbid conditions, that may have pre-dated the onset of AN – e.g. OCD, ASD, mood disorders etc.
Culture does play a role in AN – in the form of the way that it presents. We know that AN exists in non-Western cultures – where sufferers explain their behaviours on the basis of religion and/or asceticism. But religion doesn’t cause AN any more than does (e.g.) the media.
Just out of curiosity, would you generalize your above statements to BN (and/or ED-NOS) as well as AN? I am not as familiar with the non-fat/weight-phobic variant of AN as you are, though for anyone reading, here are some interesting papers on the topic – if anyone wants the full text, I’m happy to share; let me know.
Lee, Ho & Hsu (1993):
A mixed retrospective-prospective study of 70 Chinese anorexic patients in Hong Kong …41 (58.6%) of them did not exhibit any fear of fatness throughout their course of illness. Instead, these non-fat phobic patients used epigastric bloating (31.4%), no appetite/hunger (15.7%) or simply eating less (12.9%) as legitimating rationales for food refusal and emaciation. Compared to fat phobic anorexics, they were significantly slimmer pre-morbidly (P < 0.0001) and were less likely to exhibit bulimia (P = 0.001).
^ that in particular interests me, as that has been my impression from the (admittedly, few) non-fat-phobic AN individuals I’ve known or known of.
As non-fat phobic anorexia nervosa displays no culturally peculiar features, it is not strictly speaking a Western culture-bound syndrome, but may evolve into its contemporary fat phobic vogue under the permeative impact of Westernization.
I agree. However, this means that the subjective experience of the individual with the ED DOES have great significance – or in, um, personal anecdata: I remember clearly feeling that my weight was OF UTMOST IMPORTANCE, becoming almost hysterical at any mention that I would have to gain weight. Really embarrassing memories, e.g. screaming at people that asking me to gain weight was akin asking me to amputate my limbs, and HOW THE HELL WAS I SUPPOSED TO LIVE WITHOUT THOSE? THIS ANALOGY TOTALLY MAKES SENSE, OKAY, WHY DOESN’T ANYONE UNDERSTAND ME – I can laugh at the ridiculous overwrought-ness of this in retrospect while having a renewed respect for just how crazy malnutrition and impaired cognition can make someone. Even while aware I was making little sense at the time – why is this so damn important, who cares – those kinds of thoughts featured so overwhelmingly that it’s only in retrospect & with greater health that I can look at it and go, Wait, what the hell was I talking about? I remember very vividly believing that if my weight went above a certain #, I would be compelled to kill myself. And being totally shocked, upon being made to gain, that I was well above that # and the world did not end, neither did I particularly feel like dying. But at that time, those beliefs (and others) were both incredibly real, imperative and salient to me. And any attempts to dismiss or counter those beliefs were pretty summarily rejected. I found it comforting to know about the physiology of starvation and generalize those phenomena to my experience, but I also had trouble applying that knowledge to my situation. (This speaks to why I’m a fan of the concept of anosognosia for use with EDs but also opposed to it, at the same time. But more on that later.)
Eating disorders are not known for being particularly logical…
Where the cultural noise around weight and food and body comes in & becomes problematic is when it a) reinforces that yes, my weight is a totally legit thing to be this concerned about, b) lauds behaviors like dietary restraint and exercise, and c) it makes eating disorders appear more common and less serious, because as mentioned in a comment above, who doesn’t feel dissatisfied with their body sometimes? & so on. So it’s easy to assume that the weight- and fat-related ED cognitions are the same as similar attitudes in non-ED individuals, whereas the ED thoughts are so much less located in consensus reality. We may be using the same lexicon so while the overt content may be very similar to a non-ED person, the remainder is pretty dissimilar, in the extent that it takes behaviors/thoughts to.
See also: http://www.ncbi.nlm.nih.gov/pubmed/11429983
http://www.ncbi.nlm.nih.gov/pubmed/19655370
http://www.ncbi.nlm.nih.gov/pubmed/11429985
Saren, I am inclined to think (on the basis of the history of descriptions of AN over the centuries and its different presentation in different cultures) that AN could be a biologically-based illness with no specific ‘meaning’ to it whatsoever. Culture may merely provide what seems like a plausible explanation.
An analogy is psychosis. Psychosis, like AN, has always existed in our society and is not a modern phenomenon. Some people with psychosis believe that the people they are watching on television are transmitting secret messages to them and are addressing them personally. But do we blame television for psychosis? Of course not. Television is merely an environmental outlet for the expression of psychosis.
I developed AN in the 1970s as a child, pre-puberty. My AN was non-fat-phobic in the sense of not fearing that I was fat or would look fat if I gained weight. I just knew that I ‘had’ to do the behaviours, which were compulsive. Because British culture in the 1970s wasn’t body image obsessed, I attached a different meaning to my anorexic behaviours. Mostly, I felt they were about ‘control’ – of anxiety, which is a fair assessment. I had suffered with OCD since age 4-5 years old. I felt that if the number on the scales increased that my life would spiral out of control.
Very few of the public had heard of AN in the 1970s. My parents didn’t know what it was when I was diagnosed with it at age 12. Neither did I. Nowadays everyone has heard of AN, because the media is obsessed with it, and most people seem to think that the media causes AN. But what if culture merely provides what seems like a plausible explanation for anorexic behaviours? What if the body image issues (for some people at least) are iatrogenic?
The fact that AN is almost always concomitant with anxiety, depression, obsessionality, perfectionism and emotion dysregulation, it seems unlikely that culture causes these additional symptoms. The latter are probably (at least) linked to semi-starvation, but research does suggest that a proportion of teens with AN were particularly anxious, perfectionistic and obsessional children. There is also a relationship between AN and autistic traits.
In summary: AN is seen in all cultures. It simply tends to manifest differently in different cultures.
No, I know, and I mostly agree with you on the above; I do think culture is largely an iatrogenic factor rather than a true etiological one.
I would be so interested to see if there’s such a thing as a non-fat-phobic variant of BN or AN-BP. I wonder if the distinction between fat-phobic and non-fat-phobic variants isn’t a false dichotomy. Purging is an extremely compulsive behavior for me – and in large part, I think the ascription of a fear of weight gain to the motivation for the behavior is because that’s an extremely available (i.e. the symptom pool concept) way for me to make meaning and sense from a powerful and irrational compulsion.
I guess what I’m curious about (and I’m coming from a much more clinical perspective than Tetyana; my area of interest is the application of research and translation into practice) is how one addresses that. Symptoms have meaning for the individual with the ED, even if the meaning is secondary rather than prescriptive. And I don’t think it’s possible to just ignore that meaning (or at least you’ll get nowhere fast doing that, e.g. my anecdote above: it was “real” to ME even knowing the physiological reasons for that experience!) – though the monists in the room would disagree with me on that, ha.
My mother developed AN beginning around 1969-1970, similar to you, though hers did have weight-/fat-phobic components, from what little I know (she was in the US.)
I do wish we had more clarity on the exact mechanisms and interaction of etiological factors. Many people have anxious, perfectionistic, obsessive traits and difficulty with emotion regulation as children – not all go on to develop AN. (I also think the relationship between autistic traits and AN has been overstated; unless you’re talking ONLY about non-crossover [and often “non-fat-phobic” variant] AN-R which is a not a terribly common manifestation.)
Saren: with regard to those things being important for treatment, absolutely. I completely agree. When it comes to treatment, it is useless to say, “well, suck it up, you got a bad batch of genes”. Highly heritable does NOT, mean incurable. AT ALL. I’d never want to imply that. Not for an ED. For me, reading about the genetics and neurobiology, helped me feel less guilty and stupid for restricting, bingeing and purging. But, it didn’t get me anywhere in treatment, except make me feel less awful about myself for being symptomatic.
I think that the cultural and gender issues are super important in treatment. anorexicmusings, on tumblr, reblogged my post on gender nonconformity and EDs, stating that if there was a treatment center that specialized in EDs and gender issues, she’d be there in a heartbeat.
Can I disconnect my desire to look less attractive and less feminine from the ED, no. I think my sexuality and my ED are linked, and I’m not exactly sure how. But, these things are important to address in treatment, I think, and differently for different individuals. Can I say that that desire caused my ED, no, not for me. But I’m sure that those thoughts and desires were factors that led to an ED for many others. And they are important in treatment. But, I don’t think these things are truly etiological, as you say. I guess I’m more interested in etiology, and I’m worried about blaming society/media on the etiology of EDs. I don’t deny it doesn’t help and may contribute to the illness, once it is there or beginning, but I don’t think it “causes” it. Otherwise, genes and neurobiology wouldn’t matter so much. And studies show genes matter a lot.
I agree that I think that autistic traits and the link between AN and that, is probably really only relevant to non-crossing over AN, which is a small percentage of people. So, I too agree it is been overstated, but nonetheless interesting. Must read more about it.
The relationship between AN, AN-BP and BN, with regard to fat-phobia and lots of other things, is really, really interesting to me. I think BN has much stronger links to societal pressures of thinness and yet a culture of ample food. You can be anorexic anywhere, but BN requires access to ample food.
Even if EDs were 100% societal, I wouldn’t have a problem stating that, if that was true. The point is, at the end of the day, treatment and recovery, and maximizing the health and wellness of people, everywhere. We don’t need to say it is 100% biological to legitimize it. I think that’s the wrong way to go about it. It is legitimate regardless of how biological or environmental it is. Just like homosexuality is legitimate and *real*, regardless of whether it was 100% biological, or 100% environmental (and I think the mix of genetics and environment, in homosexuality, is highly variable among people). But it doesn’t matter when it comes to legitimizing the feels that person has.
I think the same is true here. Whatever the personal experiences people have, whether they are the result of etiological or iatrogenic factors, they are legitimate and both very important for treatment, recovery, prevention, etc..
But, etiology is really important. The predisposition to an ED, is important. I think putting the blame on our Western culture is erroneous.
Saren, what do you mean about culture being an ‘iatrogenic’ factor in AN? I feel like some people with eating disorders probably over exaggerate or invent the body dysmorphic part of their disorder in order to rationalize their behaviour, and of course body image disturbances are part of the criteria so to be taken seriously clinically and generally (you don’t think you’re obese at 60lbs? you’re not a REAL anorexic). I think people focus too much at times on WHY people starve themselves, as if all AN sufferers wake up one day and think ‘My thighs are fat’ or ‘I don’t want to be harassed anymore for my womanly figure’ and then become anorexic, and if you only say to the sufferer ‘your thighs aren’t fat’ or whatever that the anorexia will go away.
Going to copy/paste my response I posted on Tetyana’s Facebook; let me know if this doesn’t answer your question.
”I don’t, ever, want to discount culture and society, and gender, but I think they are not sufficient to cause an ED. And the fear I have, is by stating that they are, one can think that by changing the society, you’ll get rid of EDs, or that those with EDs are just more easily influenced by society and the thin-ideal, which I don’t think is true.”
I totally agree with you on that. I suppose am talking less about the true etiology (i.e. true causal factors, rather than factors serving as catalyst for the disorder to manifest). Where EDs become a feminist issue for me is in the cultural response to the individual with the ED: where the (ostensible) extreme desire to lose weight and control dietary intake and focus on appearance is normalized, rather than seen for the pathology it is, and these symptoms are rewarded: “I wish I had your legs, you look like a model” to someone who’s cannibalized their muscles and had trouble walking up multiple flights of stairs, where people say “I wish I could catch anorexia, just for a week or two” and despite joking, there’s some part of them that means it, and those listening nod-laugh in agreement. “I wish I had your self-control.” Where weight loss elicits a response of “You look so HEALTHY!” because “thin” and “healthy” are conflated. Never mind if that weight loss is due to a week of stomach flu, an eating disorder, illness, grief… And why is bulimia such a shameful disorder? Why will people in treatment confess to self-starvation a million times before admitting to binging? The science answers the HOW those symptoms occur and some of the why, but feminism to me explains the reactions to the different behaviors; the hierarchy of symptoms and even of the disorders themselves – in addition to why we know what we know about them, as research and science IS shaped by social priorities and forces.
Why has ED research historically been vastly underfunded, compared to other disorders? Because it (was) a “female problem.” IT BOTHERS THE HELL OUT OF ME that one of the the predominant ways to legitimate EDs as real, serious disorders is to point out that they affect men, too.
e.g. pointing to Keys’ Minnesota Starvation Study and going “See! It happens to men to!” (And yes, I’ve done that, and I probably will continue to use that as a rhetorical device because it’s one of the better, more understandable to the layperson examples we have of the major role physiology plays in producing the hallmark symptoms of EDs. But it still bothers me that I have to use MALE EXPERIENCES because culture devalues female ones. The fact that you think your personal experience and opinions are valid enough to publish via SEDs and worthy of anyone’s consideration: a result of feminism!)
I too HATE the “silly girls on a diet to look like celebrities”, EDs-as-solely-and only-psychodynamic trope. But that’s emphatically NOT what feminism has to say about eating disorders – the feminist perspective on EDs (or much of it, anyway) developed as a response to that discourse. It’s sometimes kind of a subtle distinction, similar to George & Franko, 2007: “Poor body image among some Latinos may result less from adoption of American thinness ideals, but rather from attitudes and behaviors that devalue the characteristics of Latino appearance [in addition to Latino/a identity in general.]” Does that make sense, the parallel I’m trying to draw? Body image crap is merely a symptom of misogyny and objectification of women’s bodies endemic to our culture. Body image distress =/= clinical eating disorder, of course, but there is some interesting overlap in how disordered attitudes and magical thinking have become normalized, i.e. in the “fantasy of being thin”: http://kateharding.net/2007/11/27/the-fantasy-of-being-thin/ and that is a factor that serves to perpetuate the disorder by making it that much harder to detect and that much easier to be in denial or ignorant about – both the individual with the ED and those around them, including clinicians. Those doctors that tell a parent that their child’s ED is “just a phase.” Insurance companies denying necessary treatment. A mother who praises her anorexic daughter for making “such pretty salads” because of her own complex relationship to her own weight. A culture that gives the underlying etiology an awfully good chance to manifest in this specific weight/body/food-focused way.
I love the science, I think it’s fascinating, but as soon as you move beyond a purely materialist ontology, you’re into social construction, whether you like it or not XP and I think it’s worth exploring further WHY you relate to your body in the way that you do (since we don’t know enough yet of the exact biomechanisms that might explain it) but that’s my unsolicited two cents and a personal decision. I think where you and I are is the sort of end-stage of an ED that’s persisted over a large proportion of the lifetime, where the behaviors and compulsions have long ceased to be “about” anything but themselves. I have a really difficult time relating when people talk about their ED being “about” x, y or z. It gets distilled down to a tautology, “I do these things because this is what I do.” I intellectually could name factors and insights into the reasons behind that, but it’s rare that they have emotional salience to me.
I don’t disagree with any of your points above! Only your statement that feminism has nothing to do with EDs – which is distinct from “I personally don’t find it relevant” or “that particular line of exploration doesn’t interest me.” Which…may have been what you mean, Facebook not exactly being conducive to complex discourse. To me, anything that disproportionately affects women is a feminist issue.
(And I would argue just as vehemently with the other camp, i.e. NEDA’s totally awful literature on EDs that they distribute, the failure that is usually ED awareness weeks, etc. that propose that loving your body and raising positive body image will cure or prevent a majority of EDs. Fuck that noise, yo.)
Don’t have the concentration to read all that rn, but Saren I think I love you oh my gosh. You’re so articulate and interested in science of ed’s and social justice ^.^
@Sarah, this article has a lot to do with what I’m talking about: http://www.melaniekatzman.com/wp-content/uploads/2013/05/Beyond-Body-Image.pdf
Building on these themes, other sociologists and anthropologists (Banks, 1992; Thompson,
1994) argue that the image of anorexia as a transitory, self-inflicted problem developed
by young women lost in their world of fashion and calorie restricting is a belittling
stereotype that may mask women’s real worries. By emphasizing slenderness, the dominant
imagery about eating concerns misnames as much as it discounts real biases against
women and their limited access to other forms of power of self-expression beyond corporeal
power.
In calling for such a polythetic stance to diagnosis and treatment, male cross-cultural
writers are united with feminist theoreticians in urging an understanding of patients that
acknowledges societal precipitants for extreme food denial beyond caricatured cosmetic
compliance—the latter being the socially sanctioned coloring of distress and not the cause
(Russell & Treasure, 1989). Such an approach would value the authenticity of the patients’
illness experience, not merely the validity of available experimental tools. By highlighting
the need for a ‘‘shared narrative’’ in an intersubjective milieu (Miller, 1991; Lee, 1995) that
respects the communicative power of anorexia nervosa, male and female clinicians and
theoreticians in Eastern and Western countries are casting doubt on ‘‘fat-obsessed’’ models
that blind the choice of questions asked and limit the answers to be obtained. The
repetitive polling of women internationally on fat and food-focused instruments such as
the Eating Attitudes Test (EAT), Bulimia Investigation Test—Edinburgh (BITE), and the
390 Katzman and Lee Eating Disorders Inventory (EDI) may provide a false sense of knowledge as to the
motivation for women’s war with their bodies. Unexpected results, such as the low EDI
scores of East Berlin anorectic patients in Steinhausen, Neuma¨rker, Vollrath, Dudeck, and
Neuma¨rker’s (1992) study, call into question the cross-cultural validity of constructs
tapped by our most frequently used instruments. Perhaps the renewed interest in qualitative
analytic tools (Streigel-Moore, 1994) will provide a mechanism by which to examine
the deeper meanings of self-starvation and forge broader paths to recovery.
I’d love to see more of an integration of the science and physiology with this socio-cultural feminist perspective, but I guess that gives me something to work on/towards…
Keep in mind too, that heritability values are not static, at least they don’t have to be. I would be surprised, actually, if heritability was the same across the world, for AN, for example. It might change in one culture overtime, but undoubtedly, it is probably different in various cultures too. That value depends on the environment.
“Saren, I am inclined to think (on the basis of the history of descriptions of AN over the centuries and its different presentation in different cultures) that AN could be a biologically-based illness with no specific ‘meaning’ to it whatsoever. Culture may merely provide what seems like a plausible explanation.”
I agree. And my personal interest, is in the biology. The cultural differences, though very important for treatment, education, prevention, etc.. are not of my interest to me, personally. The biological aspects are much more intriguing. To me. Hence, “science” of EDs. And I agree with you, I think a lot of my fat-phobia when I was diagnosed initially, was post-hoc rationalization for the behaviours I felt compelled to do. I have relapsed in AN and had no fat-phobia, just very recently.
Now, I don’t want to discount fat-phobic or cultural differences as post-hoc rationalizations for everyone. Of course not, I can only speak about myself. But, I do think that the underlying etiology, is primarily biological. The way one stumbles upon the fact that there’s something about restriction that’s rewarding, or compulsive, or addictive, or anxiolytic, or whatever, is different for everyone. But, the experiences people have when they are sick, fat-phobic or not, are still so similar on so many levels, it is almost remarkable. I want to know why.
I think your example of psychosis is really applicable.
I followed your comment from edbites to here– this reminded me of a book we had to read class, The Spirit Catches you & you Fall Down. It’s about a young girl with epilepsy, which her parents think has to do with her having a wandering soul.
I agree that we [as patients, as a society, as parents/caregivers trying to understand] have a tendency to ascribe meaning to things that make no sense. Frequently these myths that we create, while they temporarily make us feel better/less unhinged, make it harder to address the real disease and treat it.
This happens with drug addiction too– someone [I think mocost?] recently blogged about the myths of drug addiction including the idea that tough love worked best and addicts need to reach rock bottom.
Re: not discounting fat phobia as post-hoc– I think it may play a role as a triggering event– that if someone who was biologically predisposed to spiral into an eating disorder had never felt what it was like to be un-full, they might not find it so intriguing and might never develop an eating disorder. That said, all sorts of non-diet related things also hurl people into starvation states…
100% agree with you. Completely.
Wow, thanks for this summary of Schoemaker’s paper. I have to say, the epidemiological numbers he provided look a lot more like what I’ve seen in my lifetime than Wolf’s do — if Wolf’s numbers were true, you’d think I would’ve met A LOT more women/girls with eating disorders than I have!
I liked Wolf’s book, though I don’t remember the parts where she talked specifically about eating disorders as well as I do her analysis of changing beauty standards and their effect on otherwise healthy women, and the relationship between restrictive beauty standards and women’s efforts to gain political and economic independence. I thought *that* had merit, even if everything she’s written about eating disorders is ludicrously wrong. She probably included the eating-disorder stats (wherever she got them, if she didn’t just make them up) because she was under the impression that eating disorders were the most severe form of the culturally-induced body and food anxieties of healthy women. Which is obviously wrong, but you can see how it’d be an easy mistake for someone who is not a doctor and has never had an eating disorder to make.