What is it like for men to live with an eating disorder? What is it like for men to seek and receive treatment for an eating disorder? These are the questions that Kate Robinson and colleagues asked a group of eight men who were receiving treatment (inpatient, day patient or outpatient) at two ED treatment centers in the UK. Their goal was to find out if and how men’s experiences with an eating disorder differ from women with eating disorders.
Men account for roughly 10% of eating disorder patients (when considering anorexia and bulimia, not including binge eating disorder, which is not yet part of the DSM). I suspect this number is actually higher – as less men probably realize they have an ED, admit to having an ED or seek treatment, precisely due to the issues raised in this article (and others). Given that men form a sizeable minority of ED patients, and yet many individuals – clinicians among them – believe EDs are a women-only issue, knowing and understanding the experiences of male ED patients is crucial for raising awareness, increasing surveillance and developing appropriate treatment options for this subgroup.
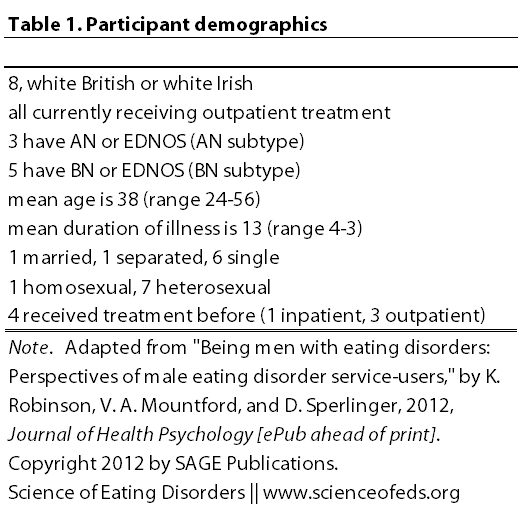
I organized information about the participants in the table below. Interestingly, all the participants reported co-morbid difficulties, most commonly citing depression (half of the sample). Note, too, the mean age of 38 years (range of 24 to 56) and the mean duration of illness – 13 years (range of 4 to 34). This sample is older than most studies I’ve reviewed thus far that focused on females. (All names are pseudonyms.)
Using the Interpretative Phenomenological Analysis technique, Robinson analysed the interviews and identified some major themes:
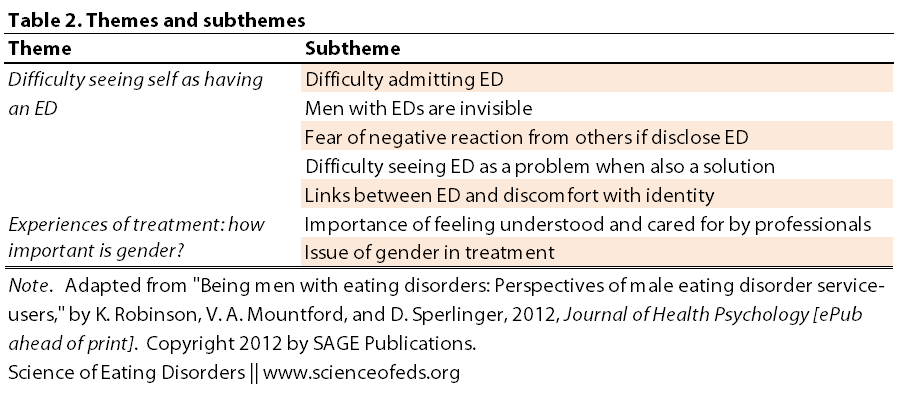
Two superordinate themes emerged (shared by at least 4 people, but majority were shared by at least 50%):
Difficulty seeing self as having an eating disorder
Some participants identified that the biggest challenge they had faced was admitting they had an ED and that it was a problem. Admitting the existence of the ED was an ongoing process and participants varied in their acknowledgement that the ED was a problem. Following the initial difficulty of admitting to oneself, they then faced the challenge of disclosing the problem to others.
Greg: It was pretty tough admitting it to myself, and then admitting it to my parents, I think the rest of it was quite easy after that.
Ed: Um … [pause] it took a lot for me to admit it. It took over 10 years for me to do it. (. . .) I think I was just a bit ashamed on the admitting side. And going for help, was just because I thought I was being ridiculous…. I knew at the time that I probably did have some kind of disorder with my eating, because being sick isn’t normal. But I’d always discount those kind of things’
However, after they found out the seriousness of the ED, and the more they learned about it, the more they were able to not only admit it was a problem, but also seek help. Unsurprisingly, they faced the same negative attitudes and lack of understanding that many female patients with EDs face as well:
Dave: (I) did a little bit of research, at least if you go in to see him (GP) with a suggestion, he’ll push it through. It’s very difficult for him at times to come up with an initiative himself because he doesn’t … he may not understand the problem then doesn’t know where to look.
Naturally, because many people believe that only women get eating disorders, the participants found it frustrating that their concerns were often dismissed or ignored. That’s why organizations like Men Get Eating Disorders Too are absolutely crucial in raising awareness about the fact that eating disorders are not exclusively female disorders.
Dave: What they see in the papers is young girls trying to get themselves down to size zero. Do you ever read about men trying to do that? I don’t. It just doesn’t get a mention. There’s no visibility there.
Frank: Most people are more socially aware than to say ‘but you’re male’ but a lot of people are surprised if you, you know, if you are male with an eating disorder … even if they don’t say so.
Many worried that if they told others about their ED, they would be seen as being weak. Of course, while this concern is very real for females as well, it is undoubtedly much worse for males, probably due to the myth that EDs are all about being slim like a model (not true!!):
Dave: If I’d been in the private sector, I think I would have probably damned my future and it’s because it’s a symptom of not being able to cope, so there’s a suspicion that on one day (…) you going to do something unusual.
Then, there’s the isolation that results from this pervasive myth:
Henry: I felt ‘I’m the only guy in the world this has happened to’. So it can be quite an isolating thought as well ‘and no other guys have had this problem. What’s wrong with me? Why have I succumbed to this if no-one else has?’
Of course, this problem extends to the scientific literature on EDs as well. Saren talked about the same circular problem that occurs with ethnic minorities that are also thought to be immune from getting EDs, in an earlier post. It goes something like this: existence of stereotypes (ie, men don’t get EDs!) –> clinicians fail to recognize this subgroup as having an ED worthy of getting professional treatment –> said subgroup feels dismissed and ignored –> clinical presentation of individuals with EDs stays homogenous –> and the cycle goes on.
Henry: All the books are directed at women which is even more ‘this shouldn’t be affecting me. This is not something I should have a problem with’.
Greg: It’s [treatment literature] all geared towards women really, yeah. I wouldn’t mind finding out a little more geared towards men really. I don’t know what the differences are, this is the thing.
I think this theme that Robinson and colleagues identified is really important and relevant not only to men with EDs, but also gender nonconforming individuals and females as well. I certainly can relate to some of these comments that the participants made with regard to the benefits of having an eating disorder (“managing stress, feeling more in control, providing comfort, suppressing sexuality, regulating distance with others”)
Greg: There was nothing else to really enjoy, and nothing else I could really control as well … it was a sense of control. I felt that my eating was like an outlet, it just made me happy.
Frank: Part of the thing that I really value about being underweight is that is suppresses my sexuality.
Here are some personal thoughts I’ll share, because I think it is important. I can really relate to Frank. Honestly, it is just so nice to have that out of the way when your natural libido levels are high. Nevermind that amenorrhea also makes life so much simpler. For me, too, one of the things I really enjoyed about being underweight was not being noticed or seen as physically/sexually attractive. That feeling has gotten better in the last 1-2 years, perhaps due to being in a long-term serious and absolutely amazing relationship, perhaps for other reasons. I’m not entirely sure. But, I definitely hated any kind of sexual attention, particularly from the opposite-sex, in high school and my undergraduate years. Weight loss removed that. I was too thin to be sexy or attractive. I loved that.
I felt uncomfortable in my naturally curvy body, but, for me, this stems from that body being seen as “sexy”, especially by males, in our culture. In retrospect, I think this came from wanting to feel equal. And I didn’t, and, frankly, I still often don’t. Getting rid of my curves meant being listened to for what I have to say, and what I have to say only. I think these things played into my eating disorder (as well as my sexual orientation). But I’m not sure. It didn’t start it, it didn’t continue it, either, but, it played some role in the whole process. Without these feelings, I’m sure I would have still had an ED. But, it is a part, maybe a very small part, but a part of it nonetheless.
Unsurprisingly, Robinson goes on to say that “participants had various struggles with identity conflicts around their gender identities, sexual identities, who they were and their acceptability”. It is a common theme, I find. Certainly not for all. I would think it is probably not even true for a majority (just a guess!), but, it is a theme that definitely needs to taken into consideration when thinking about treatment. EDs that are accompanied by gender or sexual identity issues likely require a slightly different approach to recovery than the typical fluff of “accepting your body” and you know, drawing those pictures of what you think your body dimensions are, etc. etc..
These themes don’t disappear for men:
Anthony: It’s like girls, there’s a lot of competitiveness. Um … try to look the best, trying to have the best bodies. That’s why I think women and gay men are quite similar in eating disorders, and in image and things like that.
Greg: Because I used to be really big, you know, people used to stare at me. So I don’t really want to go back to that. So this whole thing has been, the whole maintaining it and trying to look a certain way.
Experiences of treatment: how important is gender?
This is an interesting summary on this superordinate theme from Robinson: “There was a lack of consensus on whether gender was relevant in treatment, even within the same participant [italics mine]. An ED was thought of as rendering gender irrelevant yet there were examples of different issues for men and women with EDs, and difficulties with mixed sex treatment environments.”
In general, the concerns expressed here were similar as those that females often voice: a.) treatment is not long enough, b.) doesn’t offer enough, c.) professionals/treatment team often do not understand, or worse, d.) do not listen to them!
Take note professionals:
They often felt that professionals did not understand what was being asked for and they were given something that was not wanted or not given anything. What was offered was sometimes thought of as unhelpful (e.g. painful/traumatic), or reinforcing previous life experiences. If they had felt uncared for in their lives, it seemed that they sometimes felt similarly uncared for by professionals: ‘I didn’t come out feeling full of joy and happiness “oh I’m being sorted out” sort of thing … more like “10 minutes of his life [the professional] he won’t get back”’ (Henry)
What about the role of gender in treatment?
Robinson reports that participants often felt conflicted. Some felt that having an ED makes both genders more similar than different, and that they face similar challenges in treatment and during recovery. Some also felt that *everyone* was different and unique, regardless of their gender, so an ED is not the same for any two people.
Like many females, they raised the concern of “having many people with EDs together was.. more detrimental”. EDs can be very competitive, even in a treatment setting with most individuals truly wanting to get better.
But, some participants did raise important issues about what it is like to be the only man in treatment with women:
Bill: [As the only male] you become aware of people holding back or you being purposely excluded, or people saying ‘maybe it’s best if you’re not in this group because …’
The groups I’d be sitting in on … on the ward with all the women … body image things, they really didn’t bear any relation to … the issues that I had. And also cultural issues as well, because a lot of the time there was this unspoken thing, ‘because we’re women we’re expected to be slim’. I know that wasn’t the issue. That’s never really the issue for eating disorders … it can be a driver I suppose, but that wasn’t for me.
I think it is interesting to see the similarities and differences between what men and women typically experience during the course of their eating disorder, with respect to coming to terms with it, coming out about it, and experiences in seeking and receiving treatment.
This entry is getting long (I’ve been trying to keep them short and failing badly) and I’m tired (truth).
So, to wrap it up, I’ll share Robinson’s summary:
- male-specific issues included: “the difficulty of EDs being thought of as a female problem”
- common themes were also present: “ED as both a solution and a problem”
Participants were not uniform in their perspectives and it must not be assumed that there is a unitary presentation of EDs in men (duh!). The findings also demonstrate the need to raise awareness of EDs in men: among professionals to facilitate detection, within society to decrease men’s fears of a negative response and among the men themselves to assist in the process of admitting that there is a problem. Although EDs affect many fewer men than women, it is important that this minority population is not overlooked.
Ditto.
Readers: what are your thoughts on some of the concerns and feelings raised by the participants? Have you been in treatment with males? If you are a male with an ED, please share your experiences on any of the issues raised in this article (or any other relevant issues!). It is so crucial (and remember, you can do that completely anonymously).
References
Robinson, K., Mountford, V.A., & Sperlinger, D. (2012). Being Men with Eating Disorders: Perspectives of Male Eating Disorder Service-Users. Journal of Health Psychology PMID: 22453166
Definitely agree with using the ED as a means for suppressing one’s own sexuality as well as (perceived) sexual attractiveness to others. This goes for males AND females. I can’t tell you how many people I’ve spoken to- of any gender- that said that being sexually ‘unattractive’ either made them feel ‘safe’ from being re-victimized (i.e. they felt like sexual predators would not be attracted to them), and many felt that they were likely to act out sexually (usually related to earlier sexual trauma) if they were re-nourished.
I’ve also heard plenty of people that assume that if a man has the desire to be thinner, he MUST be gay. And there are men that are afraid to speak up about their ED because they are afraid that people will make that assumption about them. Of course, it’s a total myth, but that just goes to show how much room there is for increased awareness!
Joy: I completely agree with you!
And yes, there’s a lot of room for increased awareness, and even more room for knowledge.
Hey Tetyana,
I was googling 5-HTP one day and one of the search results was a bodybuilding forum thread.
The vast majority of members of this forum site were males, “dude” types who used a lot of bodybuilding jargon and seemed if anything to be hyper-masculine.
It turns out that a lot of these men suffered from either BED or bulimia. Some were more open to admitting it than others, some continued to justify the practice as part of their fitness regimen (at least, in the moment during which they wrote the post I was reading — maybe the downward spiral had yet to begin fully. I too remember a day when I wanted to continue with bulimia as a weight management ‘strategy’).
These men were NOT in treatment, from the sound of it. They were on a bodybuilding forum site, asking their peers:
— Have you ever experienced this weird binge eating I’m going through?
— I’m frightening myself, how can I stop?
— I’m purging, what’s going on here?
A common bulk-building strategy is to gain a lot of weight through anaerobic weight-lifting and a high-calorie, high-protein diet, and then to “cut” — which means to cut your calorie intake by about half (for a large male) in a very short period of time to force your body to lose weight rapidly and achieve a chiseled, but very lean, look.
As you can imagine, the “cut” period involves severe dietary restricting, which leads to bingeing, which leads to panic, which leads to purging… etc.
Anyway, these men will probably never make it into the clinical literature, but I think this is a growing subculture that even many ‘normal’ (ie, non-body-building) males are dabbling in.
I’ve never felt that body image was the primary driver for my ED, and I think that’s the case for many other people, including these body-builder guys. Body image may be one part of it, and another compounding factor is the objectifying approach we take toward the body:
— It is a ‘machine’ that I can tweak through this bulk-build-but strategy
— It is a tool that I can use to manage my sexuality
— It is an object that I can manipulate to play out my need for control and stability in a chaotic inner world (describing my own experience)
An ED is so complicated! This we know. So of course, body image + body objectification + psycho-physical stress… these still only make up part of the equation. The key takeaway that your summary points out, and that I saw validated in those forums, is that none of these factors are gender-specific, or really exclusive in any way.
I love that you wrote about this — thank you as always for being so dang thoughtful and smart! 🙂