Symptom fluctuation and diagnostic crossover are common in eating disorder patients. A study by Eddy et al. (2008) – who followed patients over an average of 7 years – showed that crossover between subtypes and full-syndrome diagnoses is very common : of those initially diagnosed with anorexia nervosa, almost 73% crossed over to another diagnosis (between symptoms and to bulimia nervosa). More specifically, roughly 50% experienced fluctuation between subtypes (restricting, AN-R, and binge/purge type, AN-BP) and roughly 35% crossed over to bulimia nervosa (a subset experienced both). Of those initially diagnosed with bulimia, roughly 14% crossed over to AN-BP and of those, 3.91% crossed over to AN-R.
This finding (though, well-known to ED specialists and even more well-known to patients) has important implications for treatment. For example, CBT and anti-depressants seem to have positive results in bulimic patients, but not so much in anorexics. What then, about those that crossover from AN-R/AN-BP to BN? Would they, too, benefit from these interventions?
In order to answer those questions, it would be helpful to know who whether we can actually predict who will crossover. In order words, are there any characteristic traits that correlate with a crossover in diagnosis? Tozzi and colleagues investigated this question in multi-site study that was published in 2005.
SUMMARY OF FINDINGS:
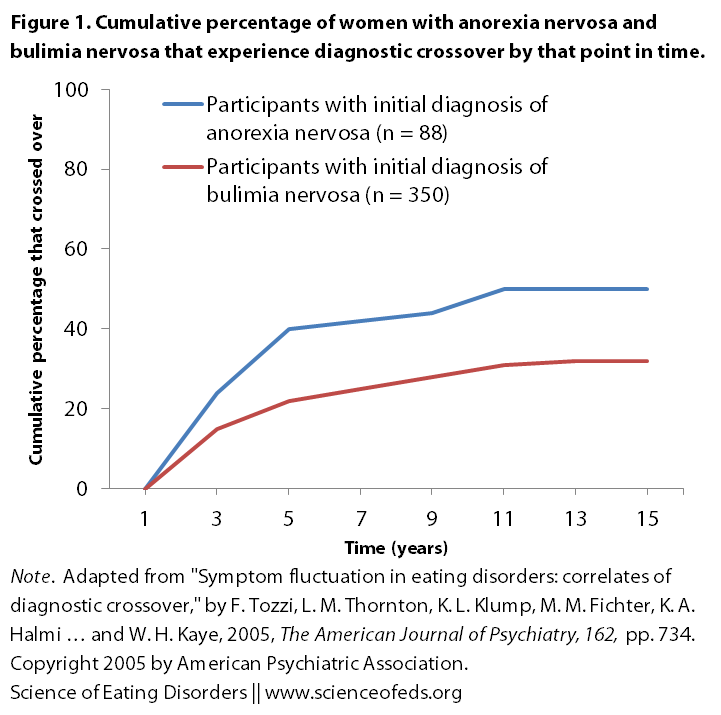
- 36% of those with initial diagnosis of AN-R developed bulimia nervosa, 91% crossed over in the first 5 years of the illness
- 27% of those with bulimia developed AN-BP, 77% crossover over during the first five years
CORRELATES OF CROSSOVER:
From anorexia nervosa to bulimia nervosa
- low self-directedness
- high parental criticism
- neuroticism
- trait anxiety
- depression
- substance abuse
From bulimia nervosa to anorexia nervosa
- low self-directedness
- low novelty seeking
- high harm avoidance
- alcohol abuse/dependence
- avoidant personality disorder
Bold points are strongly correlated with the crossover. This is a graphical representation of the time-to-crossover (based on self-reports):
The authors used various questionnaires to evaluate these traits. To evaluate temperament and character they used the Temperament and Character Inventory (TCI). I’m not a psychologist, so I’m not particularly familiar with these questionnaires and what they assess, but I did find a nice description on this site, here:
The TCI is a set of tests designed to identify the intensity of and relationships between the seven basic personality dimensions of Temperament and Character, which interact to create the unique personality of an individual.
Temperament refers to the automatic emotional responses to experience and is moderately heritable (i.e. genetic, biological) and stable throughout life. The four measured Temperament dimensions are Novelty Seeking (NS), Harm Avoidance (HA), Reward Dependence (RD), and Persistence (PS).
Character refers to self-concepts and individual differences in goals and values, which influence voluntary choices, intentions, and the meaning and salience of what is experienced in life. Differences in character are moderately influenced by socio-cultural learning and mature in progressive steps throughout life. Character takes into account the psychology of the development of personality. The three measured Character dimensions are Self-Directedness (SD), Cooperativeness (CO), and Self-Transcendence (ST).
Results from Tozzi et al suggest that self-directedness is common predictor of crossover for AN –> BN and BN –> AN. Indeed, from the characteristics evaluated, only self-directedness is common to both crossovers. But what exactly is it, and what does this finding suggest?
From the site above:
Self-Directedness quantifies the extent to which an individual is responsible, reliable, resourceful, goal-oriented, and self-confident. The most advantageous summary feature of self-directed individuals is that they are realistic and effective, i.e., they are able to adapt their behavior in accord with individually chosen, voluntary goals based on a realistic assessment of facts. Individuals low in Self-Directedness are blaming, helpless, irresponsible, unreliable, reactive, and unable to define, set and pursue meaningful internal goals. Such poor resourcefulness and unrealistic behavior are often disadvantageous to the individual.
Tozzi et al hypothesize that “individuals with low self-directedness, independent of diagnosis, may be characterized by an inability to regulate behaviors and affect adequately.” This may then lead to alternation between restraint in restricting anorexia and impulsivity in binge-purge type anorexia and bulimia nervosa.
High-parental criticism was associated with crossover from anorexia to bulimia:
This finding is noteworthy given early observations of family environment across eating disorder subtypes, suggesting that families of individuals with bulimia tended to exhibit greater conflict and disorganization and less cohesion than families of those with anorexia nervosa (56), that mothers of individuals with bulimia nervosa were reported to be more domineering and have higher expectations of their daughters than were control individuals (57), and that women with bulimia nervosa reported maternal deficits in nurturance and empathy (58).
Our findings also corroborate those of Strober et al. (4), who found low levels of parental empathy and affection to be significant predictors of the onset of binge eating in women with anorexia nervosa. These observations are particularly noteworthy, given the finding in expressed emotion research that maternal critical comments are strongly predictive of treatment outcome for adolescents with eating disorders (59).
I am kind of fascinated by this finding. In part because I keep reflecting back on my eating disorder trajectory and family life. I suppose I’m surprised at the fact that it seems to be a very important predictor of crossover, specifically from AN to BN. I guess I didn’t think it would be so important? Readers, what do you think?
Predictors of crossover from BN to AN (particularly low impulsivity and novelty-seeking) are to be expected. Anxiety was not found to correlate with crossover in this study, though previous studies have suggested that it is important in predicting crossover from AN to BN. Tozzi et al suggest this discrepancy may be due to the use of different methods and tests to evaluating anxiety.
Some limitations of the study to keep in mind, I think 2 and 5 are particularly important:
- (1) inability to examine all possible diagnostic crossovers;
- (2) 57% of those with AN and 38% of those with BN were evaluated before the fifth year of their illness and thus might not have reached their “steady state”, as Tozzi et al. write;
- (3) limited/no details about changes of severity in illness (partial/full recovery between AN and BN? – I had partial remission from AN, prior to onset of BN, which led to AN-BP and then back to AN);
- (4) no data on childhood psychiatric disorders and sexual abuse (previously shown to be important predictors);
- (5) “onset of diagnoses and determination of crossover were based on retrospective reports and may be subject to recall bias”
The authors suggest that given the fact that “low self-directedness has been associated with a negative outcome.. [and] high self-directedness predicts rapid and sustained response to CBT in BN patients,” treatment approaches would be wise to utilize methods of increasing the levels of self-directendess in patients.
I definitely think this is true – recovery and remission, for me, is always associated with generally behaving much more responsibly and reliably. I’m generally a goal-oriented individual, but that definitely has fallen to the way-side in the past, when bulimic symptoms were particularly dominant. I think things have never gotten that bad precisely because when my ED starts interfering significantly with my goals, directly or indirectly, it motivates me to really focus on reducing symptoms, which then gives me more time and mental energy to be more involved and this further helps recovery.
Readers, I’d love to hear any thoughts you have on these findings? Do you think they make sense and are they representative of your experiences and observations?
Side note: I’m sorry for the delay between my previous post and this one. Social life sometimes get in the way, which is, frankly, pretty awesome. I’ll try to make another post tonight or tomorrow.
References
Tozzi F, Thornton LM, Klump KL, Fichter MM, Halmi KA, Kaplan AS, Strober M, Woodside DB, Crow S, Mitchell J, Rotondo A, Mauri M, Cassano G, Keel P, Plotnicov KH, Pollice C, Lilenfeld LR, Berrettini WH, Bulik CM, & Kaye WH (2005). Symptom fluctuation in eating disorders: correlates of diagnostic crossover. The American Journal of Psychiatry, 162 (4), 732-40 PMID: 15800146
I find this really fascinating as well. I was first diagnosed with AN-R as an adolescent and struggled for about 7 years, experienced partial remission before going off to college, and then started bingeing and purging my sophomore year in college. I have been struggling with AN-b/p ever since (I am 28 now). My bulimic symptoms have been pretty severe ever since I started b/ping, but I always think I still identify more with the “anorexic mindset.” My goal is always to remain underweight and I have a huge fear of gaining any weight that would change my diagnosis from AN-b/p to BN. I also tend to be more like the “stereotypical anorexic” in terms of personality than the “stereotypical bulimic” (silly stereotypes, not sure how much research there is to back them up)– shy, reserved, perfectionist, NOT impulsive at all, etc.
Anyway, I really identity with the “low self-directedness” thing, and actually think it explains what was going on when I crossed over to bulimic symptoms. I was experiencing a lot of self doubt and confusion about my life and my future goals. What I THOUGHT I wanted for my life, I suddenly wasn’t so sure about. I felt like I was letting my parents down because I didn’t know exactly what I wanted to do with my life, and thus started b/ping and of course that only made it all so much worse… ended up taking many medical leaves to go to treatment and taking 8 years to graduate from college. :/
I’d be interested in more studies that looks at specific differences among people of various diagnostic patterns (i.e. are people with BN who started off as AN somehow different from those who were always BN? What makes some people with AN-R never cross-over to AN-b/p or BN?, etc.). It IS confusing when I hear professionals talk about “what works for such and such eating disorder” because I always wonder where I fall on the spectrum… maybe the “standard” treatment for b/p behaviors (“just take Prozac!” ha, tried it with no luck!) doesn’t work on me because I was a restricting anorexic first, and still identify more with that eating disorder?
Great post, great blog!
I thought “perfectionism” was a common trait among bulimics, too?
Lea: from my readings, yes, that does seem to be the case. However, this study just looked at the predictors of crossover from AN to BN and BN to AN. So, they compared perfectionism, and other scores, in AN–>BN vs. AN-only groups an BN–>AN vs. BN-only groups. Does that make sense?
Hi Becca, thanks for your comment!
What you say makes a lot of sense to me, and I can relate to some extent as well. I think the impulsivity trait would vary depending on things like: are all of your binges/purges pre-meditated and planned, or are they spur of the moment? Do they occur because of really heavy restricting or even when you eat normal meals (and consume enough calories (proteins, carbs and fat))?
Personally, my answers to those questions, as well as the other components of “self-directedness”, would have varied over the last 5+ years, depending on what else was going on in my life.
Awesome questions but really hard to research for a few reasons. Namely, what’s the difference between cause & consequence, premorbid factors or early stages of the disorder or scar-effects? Hard to untangle that, particularly when the rates of EDs are quite low. You can try to see the differences between those with AN-R and AN-BP and BN, like this study, and others, but that doesn’t answer the question of: are these traits stable? I’d bet many aren’t (given the high rates of crossover suggested by Eddy et al., 2008 and Eddy et al., 2010 studies – check out earlier posts for that). Moreover, these differences don’t explain *what* makes people cross-over.
I suppose the prevalent opinion is that those in the middle of the two extremes (AN-only and BN-only) fall in the middle, in terms of characteristics and traits that are typically more associated with either disorder. I’ll look for studies, but, I’m uncertain I’ll find anything, because you do need quite large numbers to be able to detect a real difference, as oppose to just a false positive. Even in this study, they looked only at the AN–>BN and BN–>AN crossover, not differentiating between AN-restricting and AN-binge/purging.
I wonder if Eddy et al., collected the data on personality and psychiatric comorbidities. That would be interesting to look at it.
How are you doing, Becca? I can relate to so much of what you’ve said. My diagnosis is AN-B/P. It was AN-R for 10 years. It was the AN-mindset that took over with purging one of the times I tried to re-feed after sever restriction going back to college. The slow digestion, reflux, and a medication change also had something to do with it. It’s the same disorder it’s always been, just more health problems due to years of abusing my body, more longterm effects probably in terms of brain chemicals too (making it harder to break out of this pattern) and I feel my ED only got more “vicious” toward me and others as time progressed. Otherwise it’s still fear of feeling the sense of being in a grown-woman’s body that drives me to restrict so much, then binge and purge. “Perfecting” the bingeing and purging so as not to gain weight only led to more loss of control, more loss of myself and my life, many near-brushes (real) with death and traumas for my family, and in the end, whether you binged and purged it or just restricted, you’re back to that starvation mode every night—a cold different from normal cold, a cold to the core, a cold from the inside. Feeling depressed and hopeless sometimes for no reason other than physiologically due to malnourishment. Wasting years in treatment and never experiencing the full wonders of life. You either get better, or the disorder gets better. But the disorder only wins if we lose, everything we care about and want in life.
Can relate to wondering which disorder I have, and constantly trying to “figure out” what fuels it the most.
And fear (ED’s fear?) of being diagnosed as BN instead of AN-B/P keeping me from trying to quit the purging “unless” (insert triggering ED rule here)… so I’m trapped.
Here’s my belief though. Bingeing and purging is a natural progression of anorexia. And no “eating disorder” is so different from another because the mental part is so similar and you have to treat every person separately, based on their own emotional process and needs, the way they think, act, etc. (at least that’s what my therapist said…which made me more confident getting help from her! She seems to know what she’s doing!!!)
Good luck everyone. Wish there were a more immediate cure or preventative measure for this. It’s one of the most awful illnesses, I think.
I’ve certainly had a lot of cross-overs. Before truly admitting that I had an ED of any sort (I just deluded myself into thinking “I’m just trying to be pretty and healthy”), I didn’t know there were sub-types. Now that I know more about it, I realize that I have gone from AN-R, to AN-BP, to BN-BP, to BN-NP, to what I guess is now BED… Ugh.
That’s interesting about the self-directedness factor.
Also, as far as family issues goes, I could see the strong influence in many case, such as sparking the onset and/or compounding the exising disorder, absolutely, but I’m not sure if it really is THAT important/influential that the article makes it sound.
I have really enjoyed exploring this site today. I just wanted to note that I found antidepressants to help anorexia but not bulimia – actually taking them triggered my anorexia turning into bulimia because SSRI’s at the normal therapeutic dose increase my appetite and make me gain weight and that was very triggering. I now take a low dose of them and that helps me ride the line and not go too far one way or the other.
Thanks for your comment Katie. Interesting experience with the SSRIs — sorry to hear it triggered BN onset, but glad that you figured out a dosage that works for you!