One difficulty in measuring rates of recovery for patients with anorexia nervosa (AN) is coming up with a cohesive definition of “recovery” that most of us can agree on. Similarly, it is hard to identify whether a particular treatment course is working when the patient and the clinician have different goals in mind. A 2010 study by Alison Darcy and colleagues (article is freely available here) – in an attempt to understand the patients’ goals – aims to explore how patients define recovery and engage in treatment. This study differs from a lot of the literature on treatments and recovery in that all the data comes from individuals with a lifetime history of AN. The population sampled includes 20 women with a mean age of just slightly over 29 (range from 19-52). This is a small sample size, which can make it difficult to generalize responses, and the information gathered is biased in that it relies solely on patient recall and experience.
This paper not only touches upon patients’ own goals in recovery, but what causes them to stay engaged in treatment and what causes them to drop out. (As a person who has been in and dropped out of treatment before, I appreciate this piece of the study. I often say I stopped treatment when I did because I turned 18 and got cocky, which is partially true, and it doesn’t much matter in my life right now because I have found my way back into treatment. Nonetheless, no one ever asked why and I think the assumption is that people with eating disorders stop treatment because they don’t want to get better, but this is not always the case.)
Dropout from treatment is a major problem inherent in treating eating disordered patients and is usually viewed as non-compliance, resistance or treatment failure (Vandereycken & Vansteenkiste, 2009). Most studies that have explored dropout have focused on patient characteristics and symptoms as predictors such as the presence of binge/purge symptoms, BMI on admission, severity of eating disorder symptomatology and greater psychiatric difficulty in general, however, findings are scare and conflicting (Wallier, Vibert, Berthoz, Huas, Hubert, & Godart, 2009)… no study, to the authors’ knowledge, has qualitatively investigated the patients’ own reasons for dropout.
What little research has been done examining the treatment process from the patients perspective has primarily focused on what patients with EDs consider important to achieving recovery, which includes reasons such as, “the existence of social support, motivation to change, developing an identity separate from the eating disorder and factors relating to the therapeutic alliance” (Federici & Kaplan, 2008). This study both confirms and expands on these findings.
Finally, although much of this research was exploratory, Darcy et al do hypothesize that there would be a positive relationship between autonomy in treatment and motivation, falling in line with self-determination theory (Ryan & Deci, 2000; Vansteenkiste et al., 2005) which suggests that when a patient experiences feelings of autonomy, personal responsibility or volition, they can better engage in the therapeutic process. Experiments have shown this to be somewhat true in the case of patients with AN, but results are somewhat mixed (Vandereycken & Vansteen- kiste, 2009).
Participants were given three questionnaires to fill out and then participated in a structured interview/directed conversation allowing an exploration of perspective on treatment, dropout and recovery. The questionnaires measured ED psychopathology, motivation for change and ED quality of life and results were compared to patients currently receiving inpatient treatment for AN. The results indicate that participants in this study were still experiencing significant impairment in quality of life and health, persistent ED symptoms and were only slightly more certain aspects of their behavior.
Qualitative findings from the structured interviews have been summarized in the table below. Participants discussed treatment choice, treatment goals, definition of recovery and reasons for dropping out of treatment. Of over 20 responses, results were generalized into broad categories.
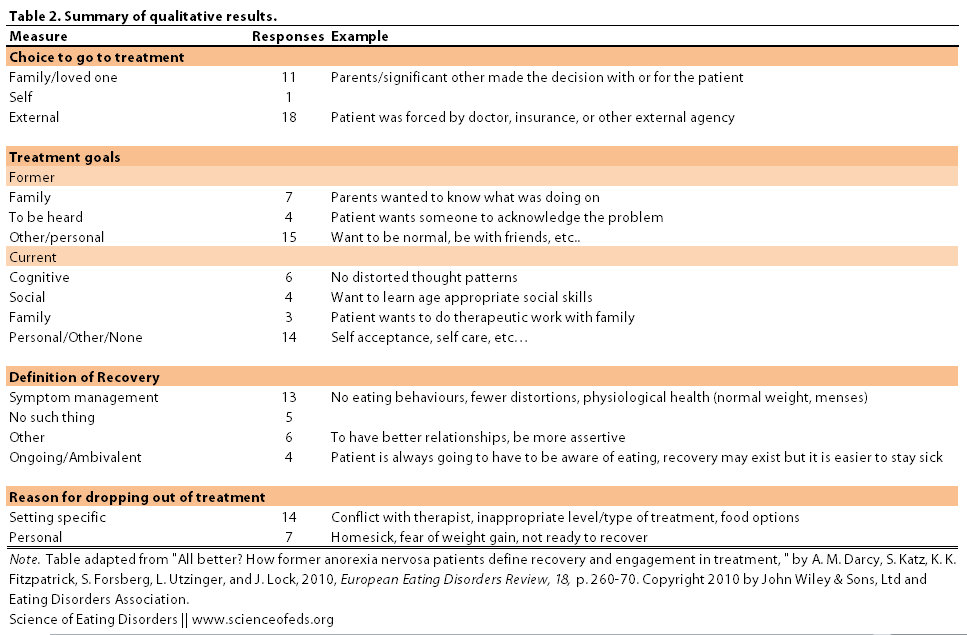
Furthermore, to test the proposed hypothesis that a sense of autonomy would correlate to better motivation, patients responses on treatment choice were used to “measure” autonomy. Results fell into two “mutually exclusive themes — either family/self (8; 40%) or external factors [i.e doctor’s decision] (12; 20%)” (Darcy et al, 2010).
Perceiving the decision to seek treatment as originating within oneself or family was significantly related to more advanced stage of change (preparation; action and maintenance). Reporting external factors as primarily important was related to current motivation in the precontemplation and contemplation stages of change. In addition, having more autonomy in treatment choice was significantly related to having an EDE [Eating Disorder Examination] score within 1 [standard deviation] of a community mean [i.e showing fewer ED symptoms].
What is interesting about these findings is that having family involvement in choosing treatment also led to feelings of autonomy and volition with regard to the choices being made. As shown, these feelings of autonomy led to increased motivation, indicated by having a more advanced ‘stage of change’. I know I’m not the only person with an eating disorder who is/has been turned-off by persistence from family. As someone who only experienced deep feelings of success/motivation in treatment when I made the decision on my own, this finding is a little hard for me to relate to. It is suggested by the authors that perhaps suggestions to seek treatment made by family members/loved ones are internalized more than those made by clinicians or health insurance companies.
Notably, one finding that speaks to treatment structure is that participants’ goals in entering treatment werenot aligned with goals often proposed by treatment providers such as weight gain, restoration of menses, etc. I’ll be the first person to say that patients with AN should not have the final say on treatment goals, but these findings suggest that“investing in collaborative [clinical] approaches to enhance engagement through listening to the patient’s concerns, and guiding them through the rational and potential usefulness of treatment,” could be a useful modification to current clinical procedures. Especially since 20% of participants cited that what they wanted most from treatment was to be heard.
Darcy et al replicated previous findings regarding what patients found to be important during the process of recovery but concluded that, “how patients operationalize at the end point of recovery is distinct from the factors they report to be important during the process.” This makes sense, for instance I think that structure – actively reminding myself of why I want health and consistent treatment support – are important at the stage of the recovery process I’m in, but in my definition of recovery, I hope that all of the things I’m doing now become less of a job and more a part of my normal routine.
Finally, it is important to note that while the most common definition of recovery stated by participants in this study closely related to commonly applied clinical definitions of recovery (including a minimization of ED related anxieties, cognitive distortions and physiological symptom improvement), there was still a great deal of ambivalence about the concept of recovery in general. Many participants didn’t think recovery existed or thought that it was a constant ongoing process:
The extensive amount of ambivalence around the concept of recovery is a concern as it suggests that it may remain intransigent even after having experienced treatment where one would expect at least some thinking around this topic. It may be reflective of an ambivalence that is a result of the illness state itself since a similar proportion of participants’ EDE scores were indicative of severity warranting a diagnosis of AN. Nonetheless, this suggests that exploring this topic itself, in addition to motivational enhancement, may benefit patients in providing a personal and meaningful focus to strive toward in the long term. In particular, some participants may benefit from learning that people can and do recover.
This paper is correct in citing such ambivalence as a concern, especially coming from patients who have received intensive treatment. It is hard to be engaged in a process if you don’t believe in the proposed outcome. As someone who has gone back and forth in motivation and on the idea of recovery, I can attest to the fact that learning that people can and do recover has changed my views of recovery. I also know that in periods of very symptomatic relapse, I tend to think that symptom management is all I want out of “recovery” and when I’m more nourished and working on cognitive processes, I want full recovery. (All of this confusion still exists in spite of numerous, different types of treatments.)
In the end, the variety of responses to all of the topics explored in this paper reflect a serious need for individualized care, as the needs of individuals vary not only within one diagnosis but also during the course of the disorder. Collaborating with the patient (when appropriate) can lead to feelings of volition and responsibility and ultimately increase motivation to change.
Editor’s Note: I (Tetyana) edited the title from Gina’s original “patients with anorexia nervosa” to “anorexics” simply to make the title shorter (and perhaps more catchy, particularly for those who may not otherwise be interested). I prefer “patients with AN” for obvious reasons (ie, anorexia is not some defining characteristic of these individuals, they – we – are more than this disorder), but I chose to go with “anorexics” mainly out of concern about title length (this was not the only change I made to the title or the post.)
References
Darcy, A.M., Katz, S., Fitzpatrick, K.K., Forsberg, S., Utzinger, L., & Lock, J. (2010). All better? How former anorexia nervosa patients define recovery and engaged in treatment. European Eating Disorders Review, 18 (4), 260-70 PMID: 20589765