Refrigerator mothers or the idealization of thin models? Toxic families or toxins in our diets? Oh, if only determining the cause (because it has to be just one, right?) of eating disorders was that simple. All behaviour has a biological basis, a neurobiological correlate. The way our brains function—and the resulting behaviours — is due to complex interactions between our genome, epigenome, and the environment. Eating disorders do not have a single cause; we cannot put the blame solely on families, or thin models, vanity or genetics.
As a science grad student, I am interested in how non-scientists interpret scientific findings on mental disorders, particularly eating disorders. With respect to eating disorders, I am interested in how patients’ understanding of the science shapes the way they view themselves and their eating disorders, as well as how it shapes their treatment and recovery.
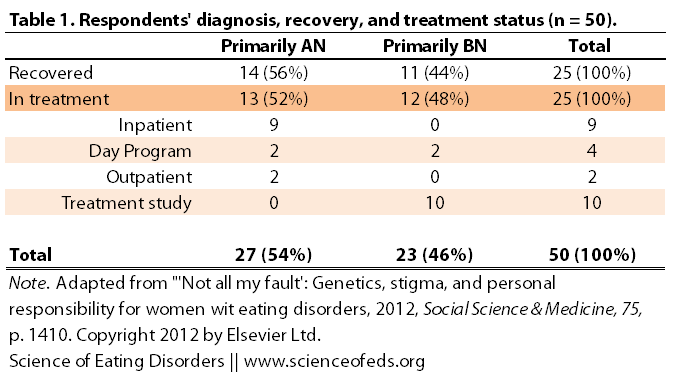
In a recent paper, Michele Easter wanted to find out just that; she wanted to know how patients with eating disorders view the increasing focus of genetics in eating disorders on ED stigma. She interviewed 50 women with a history of eating disorders, half were recovered and the other half were in treatment.
DIFFERENCES AMONG MENTAL DISORDERS
The impact of genetics on stigma seems to differ depending on the diagnosis. For some disorders, like schizophrenia, increasing the genetic contributions to the disorder seems to correlate with increased perception of “dangerousness” (Schnittker, 2008 as cited in Easter, 2008), whereas for depression and anorexia nervosa, framing the etiology with a genetic focus seems to decrease the blame and personal responsibility (as well as weakness and selfishness) that is often attributed to individuals suffering from these disorders (Winfield et al., 2011 and Crisafulli et al., 2008 as cited in Easter, 2008).
DIFFERENT KINDS OF STIGMA (IN EATING DISORDERS)
Easter identified two types of stigma that individuals with eating disorders often face:
- stigma from being perceived to have a mental illness — this type of stigma is common among all mental illnesses, labelling the individual as “different”, “not normal” and linking them to negative stereotypes (“resulting in status loss and discrimination”)
- stigma from AN/BN being interpreted as an ongoing voluntary behavioral choice rather than as a mental illness — this type of stigma is unique to eating disorders, involving a “trivialization” of eating disorder behaviours, framing them as behavioural choices as opposed to mental disorders. It is not uncommon for people to believe that individuals with EDs engage in symptoms because they are vain, want to look like models or are doing so for attention, and that, if they wanted to, they could recover on their own.
Easter excluded individuals with AN and BN who were not in treatment “to reduce the risk of harm from fatalistic interpretation of genetics.” The patient sample was mainly white (84%), between the ages of 18 to 64 (average 33), with some post-high school education and a range of treatment experiences (from none to multiple hospitalizations).
In analyzing the interviews, Easter used a broad definition of stigma, coding anything that alluded to “negative beliefs, images, stereotypes, social evaluations, and discriminatory treatment of people with eating disorders” as “stigma”. Importantly, during the interviews, no direct questions about stigma were asked, instead, questions focused on “past experiences and preferred understandings of eating disorders”.
SUMMARY OF THE MAIN FINDINGS
- 90% (45/50) thought that attributing EDs to a genetic cause would alleviate stigma
- 34% (17/50) thought it would make the stigma worse
- 12 (24%) mentioned both
- Volitional stigma: EDs are a person’s choice and/or fault, one can recover by using willpower, individuals can recover on their own, personal responsibility and guilt for having an eating disorder
- Negative stereotypes: “vain, indulgent, weird, crazy, stupid, silly, insecure, morally weak, trying to be cool”
- Genetic essentialism: gene are who we are, they define us, genes oversimplify the disorder and treatment, “bad genes” that lead to an ED could be related to other negative attributes or disorders
- Genetic discrimination: denial of health insurance, work, or education based on a genetic test that might confirm or predict an eating disorder
- Genetics as an “excuse” to stay sick
GENETICS AS A FRIEND
For most, the idea that genetics plays an important role in eating disorder etiology was viewed as being a positive factor in decreasing stigma surrounding eating disorders. In large part, this was due to the idea that genetic involvement alleviated the personal responsibility and guilt (volitional stigma) that is largely unique to eating disorders.
All names have been changes, T and R refer to “treatment” and “recovered”, respectively.
As respondents put it, rather than being “their fault,” a “personal failing,” and something to be ashamed of, genetics would provide evidence that there was “an objective reason,” “something real,” “something that does exist,” to explain their behaviors.
Jackie (T-BN) explained, “Having people realize that you really can’t help it. would do a lot for the stigma.” If genetics played a role, respondents expected less stigmatizing treatment from others….
Genetics also strengthened resistance to stigma from others. For example, Isabelle (T-BN) could say to a critical friend who saw BN as a matter of willpower, “Hey… Here’s this research… I’ve got, like, science to back me up here.”
Irene (R-BN) expected that with a genetic explanation, people would be “[f]eeling less stigmatized. Feeling less of a failure. Like ‘I’ve chosen to do this messed up thing. And, now I’m a freak.’ I think it would be helpful to them.”
GENETICS AS A FOE
Interestingly, about a third predicted that emphasizing the role of genetics in causing eating disorders would exacerbate stigma.
In reading the paper, it struck me that the fears responders had were based on the assumption, or premise, that genes were the sole causal factor in eating disorders. That’s the same problem that we’ve seen before with mental disorders (and other diseases, for example, cancer): the attempt to attribute a complex problem to one simple cause. That rarely turns out to be true, it can of course, but it is rare.
So, I wanted to respond to some of the fears the participants had – not to dismiss or belittle them, but to try to tackle some of the misconceptions and false assumptions that seem to underlie a lot of the fears.
The anticipated harms largely flowed from reductionist and deterministic theories of genetics. Notably, respondents’ own genetic theories were usually more complex, with ample roles for environment and personal volition interacting contingently over time.. Nevertheless, they presumed others to have simple theories, a presumption that has empirical support…
I also want to emphasize that I don’t mean to imply that their concerns are not valid simply because they are being too reductionistic; because even if patients with EDs understand that their disorders have a complex etiology, the public may not. That is to say, their concerns are valid not necessarily because the science is correct, but precisely because their understanding of the science or how they think the lay public will understand it, is undoubtedly probably true. And this, of course, has huge implications for eating disorder stigma.
Some feared that there was something fundamentally wrong with them that cannot be changed or altered. In other words, treatment is futile – this is forever. Others worried that genetic attribution might mean they have “bad genes”.
Some speculated further (Nell R-AN):
[I]f you have this genetic pre-disposition for anorexia, what else is wrong with you?.. [M]aybe the gene for anorexia is also close to the gene for mental illness or schizophrenia or something that people are really scared of… [W]hat if it’s related to the gene that makes you abuse your kids or something like that? Or makes you do something else in some other horrible way… that makes people scared…
The above quote is a good example of how some of the fears about attributing eating disorders to a genetic cause will increase stigma are the result of bad science education. And I by no means blame Nell here – I think her fears are warranted because even if she doesn’t think that, a substantial portion of the lay public probably DOES.
It is really important to remember is that genes code for proteins, not complex behavioural traits. There is no gene that makes you abuse your kids. It does not exist. There is no gene for anorexia or bulimia, either.
Some feared that genetic attribution would dismiss their own personal experiences, their eating disorder history and the way in which they’ve come to understand their eating disorder and their behaviours.
For Irene (R-BN), if BN were “essentially” genetic, it would supplant her personal narrative centered on childhood abuse, which would make her feel worse about disclosing it to others.
“Genetics load the gun, environment pulls the trigger.” It is not just genes,and it is not just environment. It is a mix of both – for some, genetics might be a stronger factor, whereas for others, it is environment. The idea that genetics is important does not, in any way, negate or minimize the importance of personal life experiences.
Others feared that reducing eating disorders to a genetic cause would mean that eating disorders could be “easily curable with an injection or pill”, and thus stigma would result from the belief that if someone was still sick, they were just refusing treatment. They were refusing to be cured.
They feared that genetic reductionism would “downplay individual effort in treatment and recovery”.
Taken to the extreme, even supposing eating disorders are 100% genetic disorders (and we know they are not), there are many genes involved. A drug has a specific target: a neurotransmitter receptor, or a neurotransmitter transporter protein, for example. Behaviour is a result of many complex biological interactions (genetics + environment), it is highly unlikely that a specific drug target would selectively cure an eating disorder, without affecting (much of) anything else. An eating disorder isn’t a bad infection that can be attributed to a particular virus, it is much more complex, and that usually means that treatment has to be much more nuanced and complex, too.
Wendy (T-BN) … said she was “against” the idea of a genetic explanation because it seemed to confer more blame and make the disorder a permanent and essential part of her…
“… it makes it sound like it’s my fault that I have it. Well maybe not so much my fault. But just like that’s who I am. And I don’t like that. Because I don’t see my eating disorder as who I am. I see it as something that’s, like, invaded my life and that I want to get rid of.
We are not our DNA (even if EDs were 100% genetic, which, again, they are not). We are not defined by any singular thing, be it hair colour, or skin colour, or the kind of cancer we might be susceptible to. This is true for everything, even conditions that are solely genetic, like Down’s Syndrome. None of us should ever allow ourselves to be defined by any single thing, especially, a genetic condition, a mental disorder or a disease.
Can genetic framing of eating disorders actually prevent or hamper recovery?
I think it [genetics] would have been an enabler for me. I wouldn’t have stopped the behavior. Because, I would have thought I couldn’t. I would have seen that as the reason I couldn’t. That I didn’t have control over it. (Fran, R-BN)
Delia (T-AN) theorized that her exposure to biogenetic explanations actually did prevent recovery: Well, that kind of made it easier for me to continue doing it. Because, then it took the blame off me. And, say “Oh. I can’t control this as much. Because, it’s biological. It’s in my genes. So, therefore I can’t control it.”
Eating disorders are not a solely genetic condition; we are not born with it, the way one is born with a chromosomal aberration, for example. High heritability does NOT mean little can be done to control the outcome of the disorder. I’m going to quote from my favourite webpage on this, again, because it bears repeating as a reminder for all of us:
- Heritability and environmentability are abstract concepts. No matter what the numbers are, heritability estimates tell us nothing about the specific genes that contribute to a trait. Similarly, a numerical estimate of environmentability provides no information about the important environmental variables that influence a behavior.
- Heritability and environmentability are population concepts. They tell us nothing about an individual. A heritability of .40 informs us that, on average, about 40% of the individual differences that we observe in, say, shyness may in some way be attributable to genetic individual difference. It does NOT mean that 40% of any person’s shyness is due to his/her genes and the other 60% is due to his/her environment.
- Heritability depends on the range of typical environments in the population that is studied. If the environment of the population is fairly uniform, then heritability may be high, but if the range of environmental differences is very large, then heritability may be low. In different words, if everyone is treated the same environmentally, then any differences that we observe will largely be due to genes; heritability will be large in this case. However, if the environment treats people very differently, then heritability may be small.
- Environmentability depends on the range of genotypes in the population studied. This is the converse of the point made above. However, it probably does not apply strongly to human behavior as it does to the behavior of specially bred animals. Few–if any–human populations are as genetically homogeneous as breeds of dogs, sheep, etc.
- Heritability is no cause for therapeutic nihilism. Because heritability depends on the range of typical environments in the population studied, it tells us little about the extreme environmental interventions utilized in some therapies.
There were more general fears about genetic discrimination that I think are actually more worrisome for solely genetic conditions. I think the ethical issues with regard to genetic testing and work, school and insurance discrimination are very important to discuss – and will affect us all – but, the topic is too vast and much to complex to be covered in this post, or even on this blog. Except to say, we are far away from predicting whether someone will develop an eating disorder just by looking at their DNA.
I very much liked that the sample in the study included individuals who have recovered and are in recovery from eating disorders. But, I wonder what about the rest of the population with eating disorders: those who are not in treatment, who are not white? What about males or trans people? Those with sub-threshold eating disorders?
Easter didn’t find differences between individuals with different diagnoses, different age groups or educational backgrounds, but my hunch is that is likely because her sample size was not large enough to detect some of those differences that may exist. It seems unlikely to me that there wouldn’t be a difference in the way genetic framing of eating disorders impacts how patients perceive ED stigma – between 15-year-olds and 65-year-olds, for example.
In any case, I’m interested to read follow-up studies on this topic.
It is been quite informative for me to be able to step out of my science bubble and see how the way I often write or phrase something, can be (mis)interpreted by non-scientists. It is very important for me to understand and be aware of the assumptions I am making (often subconsciously) about others’ prior knowledge. It is definitely useful in learning how to better express myself, to say what I really mean to say, and to be aware of how it may be interpreted.
References
Easter, M.M. (2012). “Not all my fault”: Genetics, stigma, and personal responsibility for women with eating disorders. Social Science & Medicine, 75 (8), 1408-16 PMID: 22819736
Fabulous – hugging your brain again for writing down what I know but am totally unable to explain.
Thank you. xx
Thanks Charlotte! 🙂
The most insightful, thoughtful, helpful reading I have ever seen on this topic, by FAR.
Thank you Laura!
Yes. It annoys me when people say that the genetic component of eating disorders means you are born with them!
Ditto.
I agree with above comments – best thing I’ve read and THANK YOU for making something my brain has struggled for so long to understand – possible for me to follow.
Anon: thank you very much!
I remember reading an article in Nature years ago discussing this in the broader context of mental illness in general – cultural context seems to be a factor (unsurprising but interesting), if I recall correctly. For example, the way schizophrenia is understood and treated in developing or non-Western countries – genetic/biomedical explanations increased stigma of schizophrenia individuals, overall.
Another article on this topic which I think is fascinating and very relevant:
Genes and Stigma: The Connection Between Perceived Genetic Etiology and Attitudes and Beliefs About Mental Illness
Jo C. Phelan, Rosangely Cruz-rojas, Marian Reiff
Psychiatric Rehabilitation Skills
Vol. 6, Iss. 2, 2002
Abstract
An increased emphasis on biological causes of mental illness has been viewed as having the potential to significantly reduce stigma. From this perspective, the current genetics revolution can be seen as a source of hope with regard to reducing stigma. However, theory and empirical research suggest that biological attributions may have complex effects for stigma, reducing it along some dimensions while magnifying it along others. In a sample of 56 residents of New York City and Los Angeles, we assess the relationship between respondents’ belief that schizophrenia (as described in a vignette) is influenced by genetic factors and several stigma-related beliefs and attitudes about the vignette subject. We find that respondents who believe the problem may be influenced by genetics are less likely to think the person did anything to cause the problem but also less likely to think the person can improve with appropriate help and more likely to think other family members may develop the same problem. These results suggest that the genetics revolution may have both positive and negative effects for the stigma of mental illness as it affects both ill individuals and their families. We suggest that it is important to attend to these effects because, at the present time, when genetic knowledge is accruing rapidly and the cultural response to these advances is evolving in turn, we may have an unusual opportunity to influence the public interpretation of and reaction to this knowledge in a way that will reduce rather than exacerbate the stigma of mental illness.
(n=56 is seriously underwhelming, but their findings are pretty consistent with the existing lit.)
Yeah, Easter talked about the differences in how a genetic/biomedical explanation alters stigma in different disorders. She echoes the abstract you quote.
It is pretty interesting and, in many ways, understandable. A lot depends on how the disorder is perceived before hand + general scientific understanding.
Thanks for the link!