Should anorexia nervosa (AN) – or subtypes of AN – be classified as part of the autism spectrum disorders (ASD)? That’s a question that has been receiving some attention in the literature in the last few years, although there are only a handful of studies, most of which are small and limited in scope (thus limiting interpretation of the results).
In the Time Magazine article “A Genetic Link Between Anorexia and Autism?” the author mentions a study – which I decided to cover today – on emotion regulation and recognition in patients with AN. It is not directly evaluating the link between AN and ASD, but it is related and a good starting point. I was originally going to write about two papers, but I will save the other one (Is anorexia nervosa a version of autism spectrum disorders?) for another time.
The study design in this paper is quite simple. Harrison et al evaluated 20 women with anorexia nervosa and 20 healthy controls on two tasks. The first task, called Reading the Mind in the Eyes (or here) (RME) was used to evaluate emotion recognition and the second, called Difficulties in Emotion Regulation Scale (DERS) was used to evaluate emotion regulation. (I’m going to do those RME tests after I’m done with the post!)
They hypothesized that individuals with AN would have greater difficulties with recognizing and regulating emotions than HCs and that there would be a correlation between emotional recognition and regulation.
Emotion Recognition: The RME Task (revised) (Baron-Cohen et al., 2001)
This is a validated task designed to measure emotional recognition. The participant is presented with 36 photos which show only the eye area of the face. Around the photos are four words and the participant is asked to select the word which most closely matches what the person in the picture is thinking or feeling. A definition handout is available if the participant does not know the meaning of a word. The task is not timed but the participant is asked to work through it as quickly as possible. Seventeen of the photos are females and 19 are males.
Emotion Regulation: The Difficulties in Emotion Regulation Scale (DERS; Gratz & Roemer, 2004)
This is a validated scale designed to measure emotional processing. The DERS is a self-report scale containing 36 items. The participants are asked to rate their responses across a five-point scale as follows: 1 = almost never (0–10%), 2 = sometimes (11–35%), 3 = about half the time (36–65%), 4 = most of the time (66–90%) and 5 = almost always (91–100%). There are six discrete but interconnected subscales that can be calculated, as well as a total score. Higher answers indicate more difficulties with emotion regulation.
The average age for the participants was in the mid-late 20’s, AN patients scored significantly higher on anxiety and depression scales, and reported more obsessive-compulsive symptoms. The mean duration of the illness was 7.2 years (standard deviation 3.2).
The results are shown below:
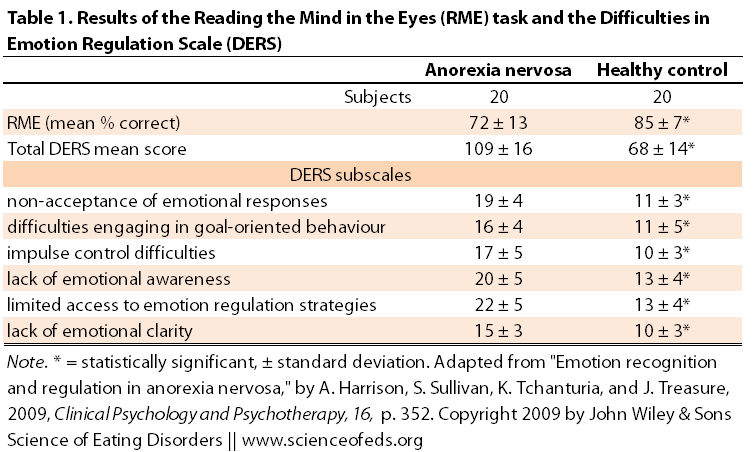
As you can see based on the t-test results, there was a significant difference between AN and HC groups for both tasks, although the standard deviation for RME, that’s the test that measures emotion recognition, seems large in the AN group. This means that there are patients with AN that score the same as or even higher than healthy controls. But on average, the AN group gets fewer questions correct. The difference seems more substantial for the DERS task that measures emotional regulation.
Harrison et al also found a significant correlation between the RME and DERS scores. That is, lower scores on the RME task (ie, less questions correct) were related to higher scores on the DERS scale (remember, higher score means more difficulties with emotion regulation). The correlation was particularly strong for the “non-acceptance of emotional response” and “limited access to emotion regulation strategies” subscales of the DERS test.
These data have been confirmed and replicated by “others” (not really “others” in my opinion, it is essentially the same group of people), but anyway, it is a different study.
Harrison et al.:
These two consistent findings highlight the parallels between EDs and autistic spectrum disorders (ASD), as discussed by Gillberg and colleagues (Gillberg, Gillberg, Rastam, & Johansson, 1996; Gillberg & Rastam, 1992; Gillberg, Råstam, Wentz, & Gillberg, 2007;) and Zucker et al., 2007. Like the ASD group, AN participants found the task more difficult than HCs. However, women with AN do slightly better than males with high-functioning autism who completed the RME task in Baron- Cohen et al.’s (2001) original study who scored a mean of 61.3% correct answers.
My initial problem with this study, before I even started reading the paper was uh… how do we know these findings aren’t due to secondary effects of starvation?
The short answer is: we don’t. Not yet, anyway. This type of study needs to be replicated with weight-restored AN patients, recovered anorexia nervosa patients, patients with bulimia nervosa, and so on.. Only then will we begin to get a better grasp of the situation. But, of course, this is a start and we have to start somewhere.
The authors actually mention this and other confounding factors:
It is possible that the findings may be secondary to severe weight loss and the starvation effects associated with AN…. Additionally, the AN group may be described as being quite a chronic group, with a mean illness duration of 7.2 years, although chronicity in AN is a poorly defined concept in itself, as Tierney and Fox (2008) discuss. It could be that greater difficulties in emotional regulation develop as the course of the ED progresses and it would be a good idea to explore this further using a sample with a shorter illness duration.
But, leaving the question of whether these results are predisposing factors or by-products of malnutrition and weight loss, they have important implications for… your guessed it: treatment.
Of particular interest here is the non-acceptance of emotion responses subscale, which… relates to a tendency towards having negative secondary responses to one’s own negative emotions or not accepting emotional reactions to distress. Evaluating emotions as being bad or wrong and the subsequent secondary emotional responses, such as fear or shame, is reported to motivate attempts to avoid emotions (Gratz, Tull, & Wagner, 2005).
Naturally, treatment approaches aimed at improving emotional recognition and regulation will likely be of benefit during the recovery process. I think strategies to improve one’s acceptance and tolerance of emotions that may be thought of as “negative”, “bad”, or “shameful” is necessary during treatment, particularly if that is something the patient struggles with. Of course, this is just one aspect of what should be a comprehensive treatment approach that – in my opinion – should happen alongside weight restoration and resumption of normal eating habits. I suspect one without the other will either lead to relapses or diagnostic crossover.
Note: There are two closely-related follow-up studies that I missed, in part because I wasn’t originally planning to write about this paper and in part because of my search terms in PubMed. Here is one and here is the other.
References
Harrison, A., Sullivan, S., Tchanturia, K., & Treasure, J. (2009). Emotion Recognition and Regulation in Anorexia Nervosa Clinical Psychology and Psychotherapy, 16, 348-356 DOI: 10.1002/cpp.628
I found this very interesting as emotional intuition and awareness (in myself and those around me) has always been one thing I had–sometimes to my detriment. I just completed the emotion recognition quiz and scored over one standard deviation higher than even the normal group. I suffer from anorexia nervosa b/p subtype. And just glancing at the list of subscales for DERS, I can tell that most of them would likely give me high scores (especially, yes, non-acceptance)….save emotional awareness. I would be interested to see a further breakdown of comparisons for these subscales.