Type 1 diabetes mellitus (DMT1) is a lifelong chronic disorder that occurs when the body is unable to produce enough insulin – a hormone that is required for carbohydrate metabolism. Patients must learn to manage their disorder by monitoring their blood sugar levels on a regular basis, carefully selecting the foods they eat and how much exercise they do. Before insulin was extracted and purified (at University of Toronto!), type 1 diabetes, which usually occurs in children and adolescents, would very quickly lead to death – the body, unable to take in the very thing it needs to survive.
Unfortunately, patients with type 1 diabetes are at increased risk of developing eating disorders or disordered eating behaviours. Diabulimia refers to an eating disorder in patients with DMT1 who reduce or skip insulin doses to reduce their weight.
The exact prevalence rates vary study by study, depending on the population sample, how disordered eating/EDs are defined and a multitude of other factors. But, nonetheless, some numbers are helpful.
Kelly et al. provide a nice overview of the prevalence studies. I’ve summarized some below:
Quick Summary of Prevalence Studies of EDs/DEBs in patients with Type 1 Diabetes
- one study suggested that the prevalence of AN and BN in patients with DMT1 may be as high as 16% (Jones & Colton, 2002)
- another study found that out of 663 patients, 5.9% had an ED (Herpertz et al., 1998)
- study of 76 adolescents with DMT1 found that 40% of females “admitted to underusing insulin to control weight” (Bryden et al., 1999)
- comparing 89 female adolescents with DMT1 with age-matched controls showed that disordered eating behaviours (DEB) were present in amount 17% of DMT1 patients and only 2.2% (still high!) of the age-matched controls (Engstrom et al., 1999)
- in another study (143 adolescents), 38% of females and 16% of males reported unhealthy weight control practices, 10% admitted to skipping insulin while 7.5% to taking less insulin to control their weight (Neumark-Sztainer et al., 2002)
There are many reasons as to why EDs and DEBs are more prevalent in patients with type 1 diabetes. It could be that, in part, due to the restrictive and controlling nature of diabetes management. Larrañaga et al postulate about some of the other possibilities:
The association of chronic illness, such as type 1 diabetes, asthma, attention deficit disorder, physical disabilities and seizure disorders, with disordered eating behavior is well known. By controlling diabetes with insulin injections, many diabetics face a constant struggle with their weight. As insulin encourages fat storage, many people with type 1 diabetes have discovered the relationship between reducing the amount of insulin they take and their corresponding weight loss. It is well-known that adolescents with type 1 diabetes tend to exhibit increased difficulty in maintaining optimal weight and also are more inclined to be concerned about their weight than their non-diabetic counterparts.
The danger of skipping or reducing insulin doses are numerous. Here are just some that were outlines by Larrañaga et al (I’ve adapted – or “prettified” – the figure):
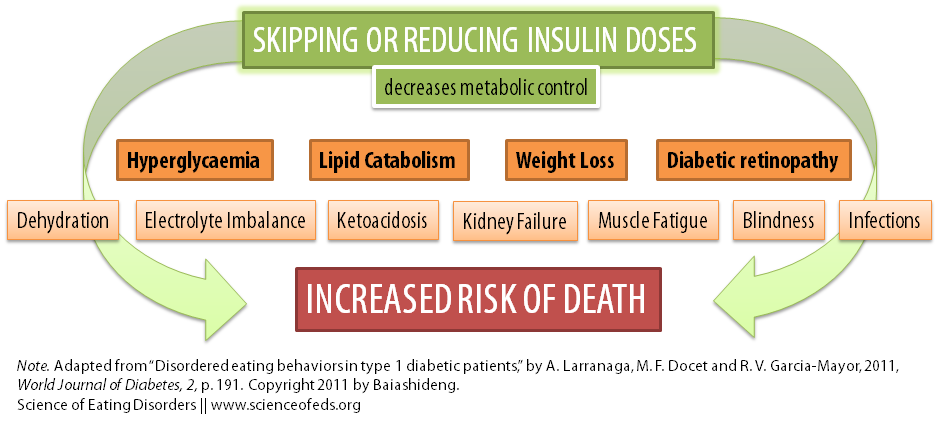
An 11-year follow up study of women patients with DMT1 found that those who restricted insulin had a three-fold increased risk of mortality. That is, the mean age of death for those that restricted insulin was 45, compared to 58 for those with normal insulin dosing (Goebel-Fabbri et al., 2008).
Treatment absolutely must consist of a multidisciplinary team including an endocrinologist of physician knowledgeable in diabetes management, a dietician (with an ED and/or diabetes training), psychologists, psychiatrists, and perhaps even a social worker, if necessary.
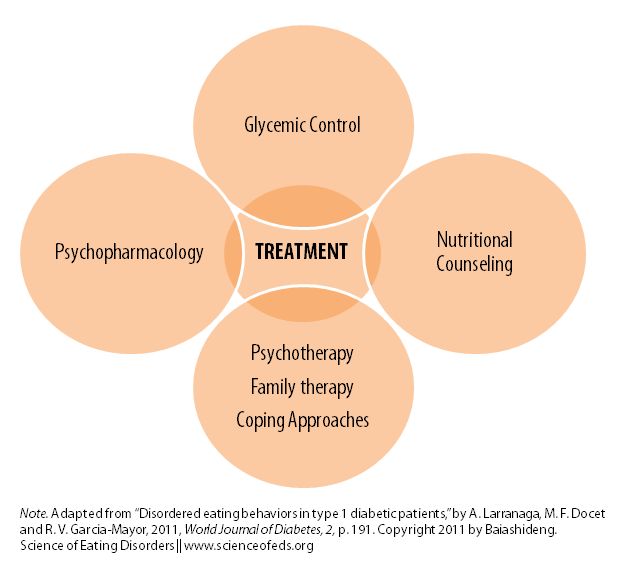
Treatment will, inevitably, vary from person to person, but, a multidisciplinary team really is a must as ED specialists may not be knowledgeable in diabetes management (unlikely, anyway) and physicians specializing in diabetes are unlikely to be aware of ED treatment, what to do, what to say (and NOT say), and so on.
Larrañaga concludes with an important message:
EDs in type 1 diabetic patients represent some of the most complex patient problems to be treated both medically and psychologically. Given the extent of the problem and the severe medical risk associated with it, more clinical and technological research aimed to improve its treatment is critical to the future health of this at-risk population.
I want to thank Claire (from Diabetes with Eating Disorders – I am assuming?) for suggesting this very important topic as a blog post idea. Fortunately, I have no experience with diabetes – as far as I know, no one in my extended family has suffered from it. So, I don’t know the reality of the day to day living with type 1 or type 2 diabetes. I want to bring the topic up on the table for discussion and I am – as always – very interested in what you have to say.
If you have DMT1 and DEB/EDs, what has your experience been like in seeking and receiving treatment?
References
Larrañaga A, Docet MF, & García-Mayor RV (2011). Disordered eating behaviors in type 1 diabetic patients. World Journal of Diabetes, 2 (11), 189-95 PMID: 22087355
Kelly SD, Howe CJ, Hendler JP, & Lipman TH (2005). Disordered eating behaviors in youth with type 1 diabetes. The Diabetes EDUCATOR, 31 (4), 572-83 PMID: 16100333
I was talking with a coworker last week about diabetes and eating disorders and she told me she was at the other end of the spectrum in college. She is also Type 1, but was a binge eater. In order to binge on candy bars, she would overdose on her insulin. Maybe not as dangerous as witholding insulin, but still very disordered.
Yeah. Unfortunately, I don’t know enough about diabetes to know if it is less or more dangerous. From my understanding – high/frequent fluctuations in blood sugar levels are not good. I can’t imagine any of it being “okay”. Yeah, I just don’t know – at all. I should read more about this, definitely.
Thank you so very much! This is a really great piece and it’s much appreciated, the more awareness the better! & yep I work for/represent DWED 😉 I’ll tweet and facebook this out from our accounts too.
xx
Thanks Claire for the suggestion! I’d love to get any comments from DWED members on their/your experiences with getting help, the reactions of clinicians, the risks, etc.. Recovery is hard because you can’t just abstain, you have to learn how to eat normally, I can only imagine how much more difficult it is with DBT1 where you still have to maintain a high level of monitoring and awareness over food and exercise.
My name is Emilee and I am 20 years old. I have had type 1 diabetes for 19 years. 9 years ago, I developed anorexia. After 4 years, I semi-recovered (I only say semi because although I became weight-restored and didn’t obsessively count calories anymore, my views on food/weight were still very disordered). I then developed bulimia. It was absolutely GLORIOUS to binge after spending so many years restricting (not just with my anorexia, but with growing up as a diabetic!). I found out 2 years later that I could manipulate my insulin for the purpose of weight loss. I felt so lucky. I didn’t have to purge anymore! It was sooo much easier.
After 2 years of constantly high blood sugars, my life was hell. I called in desperation for treatment. I had to wait 3 months for my first appointment, so I decided to tell the juvenile diabetes clinic I attended at the time about my insulin omission.
All that they provided me were looks of deep concern and confusion. They listed off all the dangers, but I already knew them. I left feeling only guilt and shame. At the ED treatment center I also felt helpless. No one on the team really knew how to deal with the diabetes aspect of my ED, and although the groups were great, I always felt alone because no one could relate to me. There were also aspects of the program that just couldn’t work for me because as a diabetic I always have to count my carbs.
At one point my health got so critical that it was suggested I go to inpatient treatment. After extensive research, though, I found that there were no ED inpatient centers that would accent me as a diabetic – it was a specific criteria for denial of admission. I felt as though I was a lost cause; that my situation was just too complex and no would could deal with me. I didn’t know where to turn, there were hardly any resources available. I wanted to give up. I was terrified, not only of weight gain, but of having to go back to constantly checking my blood sugar and giving insulin, as well as stressing about going low.
It has been 2 years since I started treatment and I am only now starting to get back in control. I no longer omit my long-acting insulin, purposefully drive my level up, or binge/omit (I only omit now if I binge/purge – yes I resorted back to purging – and my sugar spikes after).
Emilee,
Thank you for commenting. I think it is really important to get your voice heard, it is such an important issue.
I’m so sorry to hear about your struggles and the difficulty in getting proper treatment. I can’t imagine how difficult it must be, but I’m glad that things are looking-up.
You didn’t specify where you live, but have you been in touch with anyone at http://www.dwed.org.uk/?
Unfortunately, I’m not sure what resources are available for T1D patient with eating disorders 🙁
Let me know if there’s anything I can do for you.
Tetyana
Well first of all I want to thank you for posting this study!! I was almost in tears when I saw it because I’m just so thankful that this issue is getting some recognition. Hopefully one day more research and education will be put into it so that proper treatment/prevention strategies will be in place. I live in Canada, and have just contacted Claire from DWED. I hope one day I will be able to set something similar up in Canada. The bottom line is there just aren’t enough resources available but it is thanks to people like you that this will change 🙂
I’m really glad you find the information here useful! That’s my goal! We definitely need something like DWED in Canada, or at least more recognition of the issue from places like NEDIC.
Hi Emilee.
I am a representative for dwed.org.uk – the charity for diabetics with eating disorders and those associated with.
It’s great to read that you are in treatment and starting to gain back control of your diabetes and eating habits. It takes a lot of strength and bravery to take those first tentative steps. Unfortunately when you are dealing with an dual diagnosis treatment can be that much harder to access.
Many people suffering from this illness have had difficulty in finding the treatment and support they need. I very much relate to you talking about the perils of being sent back and forth between between the ED services & diabetes clinic. But don’t give up, changes are happening, gradually, it is something our charity is very much involved in and concerned about.
One thing I would suggest to you is trying to get your ED consultant and diabetes doctors in the same room, or at least in contact. They need to integrate and work together to address your condition. Also, make sure you are constantly TELLING them what they need to know. Unfortunately at the moment we can’t expect them to be fully trained in the way we ideally need them to be, but we can tell them what they need to know. Of course they must be willing to listen and understand, which is another hurdle in itself, but when you for example find an ED psychiatrist ready to go away and read and learn about diabetes it can make a huge difference.
Rambling a little here but I’d really recommend you have a look at our website, and also our facebook page. If you like I can even add you to our private group for those suffering from ‘diabulimia’/ED-DMT1 (as we term it, soon to be included in the official DSN manual too!) – everyone in the group is at different points in their illness, some fully recovered, and it is a really supportive place. I also don’t know where abouts you are location wise but the girls are from all different places so someone may be able to help you in knowing about specific local services.
I do hope this helps somewhat. The most important thing is to keep going, don’t give up. It can be easy to convince yourself not to bother when the treatment you need doesn’t seem to be there, I know, but as I said, things are changing, but we need to be out there telling and showing people how much that change is needed.
Feel free to e-mail me as well if you’d like to chat some more. I really can relate to the reactions you’ve had when trying to get help. I am in a similar situation with regards to the way I don’t specifically omit insulin so much anymore, but my binge/purge behaviours drive my levels up a lot. It can be so tough to get a hold over. You aren’t alone.
Kind regards, Claire.
If you do want to be added to our private group just send me an e-mail with a link to your facebook profile or name to search for and I shall send you an add request. No pressure though as know group settings aren’t the best means of support for everyone. Perhaps have a think about it. But like I said my e-mail inbox is always open to you, too. x
Thank you so much for your response Claire!! I would love to be a part of the private group. I have just “liked” the facebook page, so you should be able to find me from that. I think the DWED organization is fantastic – I have been to the site before and I was so happy that initiative has been taken. I am located in Canada though and unfortunately there isn’t anything set up here (I am hoping to change that though!!!) I would love to connect via email, if you wouldn’t mind sending it to me?
My partner and I stumbled over here from a different website and thought I may as well check things out. I like what I see so i am just following you. Look forward to looking over your web page repeatedly.
Just wanted to suggest a great resource for people with diabulimia: http://www.wearediabetes.org The founder, Asha, is great– she knows her stuff!
🙂
Hi everyone! I commented on this post a while back, and I made mention of how there aren’t enough resources out there for diabetes/eating disorders and diabulimia. Well, because of that I decided to found a non-profit organization called DieOrBeatThis and create a website to provide more information and support for the dual diagnosis.
DieOrBeatThis is partnered with We Are Diabetes, as mentioned in Joy’s comment above, and we work to provide ongoing suport and resources with as much comprehensive information as possible regarding all aspects of the complex combination of diabetes and eating disorders such as diabulimia.
Our site can be found at http://www.dieorbeatthis.org and I just want to welcome anyone who is struggling with diabulimia or is looking for more information to check it out 🙂
I am glad that I discovered this blog. I really love the artices you havbe on here.
I know of a simiolar blog to yours with good content about diabetes, the subject include Diabetes Diet, Diabetic Foodd and also
Diabetes Treatment, you can find the webpage here http://diabetesextended.wordpress.com. Have a nice day