It is to be expected that the Diagnostic and Statistical Manual of Mental Disorders, at least when it comes to anorexia nervosa, relies heavily on measures that are hard to quantify and measure objectively. The big exception is amenorrhea: the absence of menses (commonly known as “periods”) for three consecutive months. As I’ve mentioned before, this criterion will be removed from the next edition of the DSM, thankfully. But for now, it is still there.
Perhaps because it is easy to measure objectively, the resumption of menses is often taken to be a marker of “health” and “recovery.” It is a common goal in treatment for patients to reach a “menstruating weight.”
[Conversely, not losing one’s menstrual cycle is often perceived by the patient that they are not “sick enough.” Their eating disorder is not legitimate because clearly they are eating enough for their menstrual cycle to continue, and thus they should “snap out of it” or they “don’t deserve treatment,” which is of course not true.]
I often run into questions online with individuals in recovery who are weight restored and eating well, but still not getting their periods. They are wondering what is going? Should they eat more? Do they need to gain more weight? While such questions are unlikely to be answered (correctly) online, it did make me want to explore the topic further. I began to wonder,
What predicts the resumption of menses (ROM) during recovery from anorexia nervosa?
I found a relevant paper published 15 years ago that I am going to cover in this post. Although there have been some other papers since, few of them studied anorexia nervosa patients specifically, at least as far as I could find, and some were unavailable to me.)
Below is a simplified diagram of what normally happens, basically a lot of positive and negative feedback loops. Note that different hormones increase and decrease at various times during the menstrual cycle (for example, LH, or luteinizing hormone, peaks right before ovulation).
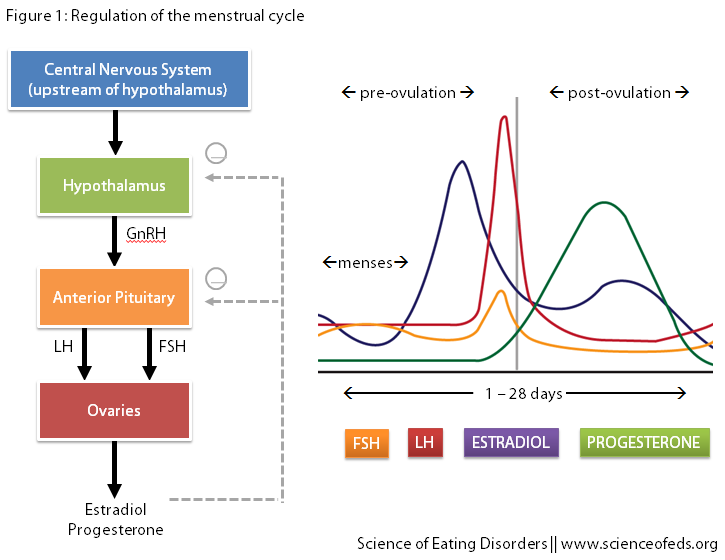
Naturally, this cycle is altered during amenorrhea, and so the authors of this study, Golden et al., wanted to see whether there are any factors that could predict or are associated with ROM. Besides looking at the levels of these hormones, the authors also measured body weight, body fat, and the levels of exercise.
This was a two year cohort study which started with 100 adolescent girls (with 69 available for follow-up after a year, and 59 available for follow-up after two years).
SUBJECT DEMOGRAPHICS
- Mean age was 17, with a range from 12-24 years
- Average weight loss was almost 30 lbs in about a year and a half
- Average length of amenorrhea was 11 months (but the standard deviation was also 11 months)
- Interestingly, 22 out of the 100 patients (so 1 in 5) experienced amenorrhea before the onset of weight loss.
MAIN FINDINGS
- After a year, 47 out of the 69 patients resumed their periods (68%)
- After two years, 56 out of the remaining 59 had resumed their menses (95%)
At the two-year mark, for the 56 that had resumed their menses:
- Total duration of amenorrhea was ~22 months (standard deviation around 16 months)
- ROM occurred around 9.5 months (standard deviation around 8 months) after patient was first seen
- ROM occurred at an average of 4.5lbs HIGHER than the weight at which menses were lost
- Mean standard body weight (SBW, taken from the median weight for height from the National Center for Health Statistics tables) at which menses were resumed was 91.6%, but the range was 75%-115%
- 48 (86%) resumed menses within 6 months of achieving a weight of 90% or above of the SBW
What about the participants that didn’t resume menses after one or two years following the beginning of the study?
Well, between the participants that did and those that didn’t, at the one-year follow up, there were no differences in weight, percent of SBW, body mass index (BMI), or percent body fat.
What about excessive exercise? At the one-year mark: 50% of subjects in the amenorrheic group were excessive exercisers, but so were 42% of those who resumed menses. Moreover, 27% of subjects who remained amenorrheic had experienced amenorrhea before the onset of weight loss, compared with 21% of those who resumed menses (not a significant difference.)
So, was there anything that correlated with and thus could predict when menses would be resumed?
Yes: levels of estradiol were significantly lower in the group that did NOT resume their menstrual cycles. 90% of patients who experienced ROM had high levels of estradiol, comparable to normal menstruating women, whereas only 19% of those who did not experience ROM did.
Note though, 10% of subjects that experienced ROM had estradiol levels lower than expected (and 19% that had high levels of estradiol still didn’t experience ROM), suggesting that the human body is complicated. (So, don’t freak out if your period isn’t coming and you weigh more than when you lost them, or vice versa.)
At the initial assessment, compared with those who resumed menses, those who remained amenorrheic 1 year later were similar in age, age of menarche, duration of amenorrhea, duration of illness, and amount of weight lost. No differences were observed in the EAT- 26 (Eating Attitudes Test), EDI (Eating Disorder Inventory), or BDI (Beck Depression Inventory) scores or in the amount of exercise performed between the 2 groups.
Something else that I thought was interesting: patients that remained amenorrheic had undetectable levels of LH during the initial visit. The chances of remaining amenorrheic were 10 times greater for those patients whose initial LH was undetectable, compared to those whose initial LH levels were measurable.
The patients in our study had been amenorrheic for an average of 21.8 months before ROM, and were therefore at high risk for developing osteopenia. Once treatment was initiated, two thirds of our patients resumed menses within 1 year. [But for some, menstrual return occurred a YEAR or MORE after reaching treatment goal weight] Our results show that a weight about 90% of SBW for age and height is the average weight at which ROM occurred and is therefore a reasonable treatment goal weight. This weight was, on average, 2.05 kg above the weight at which menses were lost…
I think one of the most interesting things in this paper is that the authors were able to predict (retrospectively, I suppose), which patients were likely to remain amenorrheic and which ones would experience a resumption of menses after one year of treatment. The group at high risk for remaining amenorrheic had lower body weight and body fat, and lower levels of GnHR (see Figure 1). As stated previously, all of them also had undetectable levels of LH at first visit.
The authors summarize,
… we found that a weight about 90% of SBW for age and height was the average weight at which ROM occurred, and 86% of patients who achieved this weight resumed menses within 6 months. Resumption of menses did not depend on the amount of body fat, but did require restoration of hypothalamic-pituitary-ovarian function, which was best assessed during follow-up by measuring serum estradiol levels.
If you are worried about why your menses are not coming, or maybe you are just curious, ask your doctor to measure your levels of estradiol (it just takes a blood test).
However, as Dr. Silber pointed out in an editorial accompanying this paper, it remains to be seen (and I haven’t done extensive research to see if this has been done already) whether “a specific level of estradiol can predict the onset of menses before periods have returned. If not, this test may be no better than asking the patients if their menstrual periods had returned. It is possible that an elevated estradiol level indicates correlation and not prediction, a higher estrogen level merely expressing a more fundamental change: the reactivation of the hypothalamic-pituitary-ovarian axis.”
From my perspective, the take-home message is that our bodies are complicated (as if you didn’t know that already, right?) and that means that no single factor (body weight, body fat percentage, BMI, caloric intake, levels of exercise, history of amenorrhea) can adequately predict when your periods will resume during recovery from anorexia nervosa. It often takes 3-6 months at a stable and healthy weight for menses to resume, sometimes even a year. For some ROM may come at an SBW of 75%, whereas for others, that may happen when their weight is 115% of SBW.
References
Golden, N.H., Jacobson, M.S., Schebendac, J., Solanto, M.V., Hertz, S.M., & Shenker, R. (1997). Resumption of Menses in Anorexia Nervosa Archives of Pediatrics & Adolescent Medicine, 151 (1) DOI: 10.1001/archpedi.1997.02170380020003
Silber, T. (1997). Resumption of Menses in Anorexia Nervosa-Reply Archives of Pediatrics & Adolescent Medicine, 151 (6) DOI: 10.1001/archpedi.1997.02170430100025
I find this really helpful, as I have always believed ROM is not an indicator of health. My menses returned and I became pregnant at less than 70% IBW!
Hi Sarah,
Thank you for your comment! I think ROM is not the only indicator of health, but is still is an indicator – particularly of bone health. But it is not the only thing. I think it is really important to remember that there is a lot of variability in terms of when people get it back, too. So, getting it back at an IBW of 70% shouldn’t be taken to mean that that’s it, you don’t have to gain any more weight. But, it might take a few months or more, at a healthy weight and calorie intake, to get it back again. Our bodies are so variable, and we are only beginning to scratch the surface of the biological basis of that variability.
The topic of unplanned pregnancies in anorexia nervosa is something I’ve been meaning to get to! Not menstruating =/ you can’t get pregnant (contrary to what a lot of people believe(d), myself included).
Cheers,
Tetyna
Tetyana, is it also possible to have your period while having an ED but be unable to get pregnant? To what extent is having a period an indication of fertility?
Good question! I don’t know! I would imagine so (perhaps fertility issues not related to EDs?) I’ll check this out! I know very little about this.
Did it matter if participants were engaged in exercise while recovering?