Excessive exercise (EE) is common among eating disorder patients. Indeed, in the study I’ll write about today, 39% of patients engaged in EE. Previous studies have tried to find psychopathological and personality correlates of EE but the results have been inconsistent. Some studies have suggested that impulsivity and addictiveness are highly correlated with EE whereas others found that anxious and depressive traits were more closely associated.
In a retrospective case series study involving outpatients with AN and BN, Penas-Lledo et al. found higher levels of anxiety and depression… among those who were identified as exercising excessively. The authors claimed that exercise might serve to reduce anxiety and stress in individuals with AN. In a similar study with adolescent inpatients with AN, Holtkamp et al. found that anxiety significantly predicted variance in exercise levels. These investigators proposed that anxiety symptoms in combination with food restriction contributed to increased levels of physical activity and that physical activity served an anxiolytic [anxiety reducing] function.
In this multi-site study, Shroff and colleagues wanted to examine the prevalence of EE across eating disorder subtypes and the personality traits and clinical variables that were associated with EE in a large sample of women (1,857 in this study).
But first, what exactly is “excessive exercise”?
Although there have been numerous studies of exercise and excessive activity in eating disorders, there is no consensus on what constitutes excessive exercise with definitions varying in frequency of hours, definitions of unhealthy preoccupation with exercise, and discomfort experienced when unable to exercise—or exercise “craving.”
In this study, participants were deemed to be excessive exercisers when they endorsed at least one of the following with regard to exercise: “(1) severe interference with important activities; (2) exercising more than 3 h/day and distress if unable to exercise; (3) frequent exercise at inappropriate times and places and little or no attempt to suppress the behavior; and (4) exercising despite more serious injury, illness or medical complication.”
PREVALENCE OF EXCESSIVE EXERCISE ACROSS ED SUBTYPES
Shroff et al. found that EE was more common among purging-type anorexia nervosa patients and least common among purging-type bulimia nervosa patients. (As a side note, non-purging bulimia nervosa means that patients binge but compensate through exercise, laxatives, diuretics, or fasting, as opposed to vomiting.)
You can see the results for all subtypes in the table below:
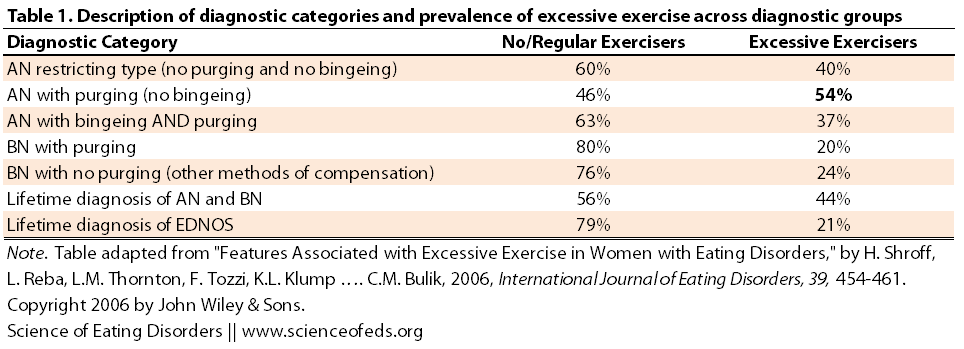
While I’m not surprised that patients with purging-type AN had the highest prevalence of EE, I would’ve also expected a higher EE prevalence among non-purging BN patients. I would’ve also predicted that non-purging BN patients would have a higher EE prevalence than purging-type BN patients. Having said that, although I never fit the criteria for EE by this study’s definition, I came closest during periods when I was restricting or bingeing/purging but considerably underweight, not when I was bingeing/purging at a normal weight (ie, bulimic).
FEATURES ASSOCIATED WITH EXCESSIVE EXERCISE
Next, Shroff and colleagues compared the “no/regular exercise” and “excessive exercise” groups, irrespective of their diagnosis. I summarized the differences they found in the table below:
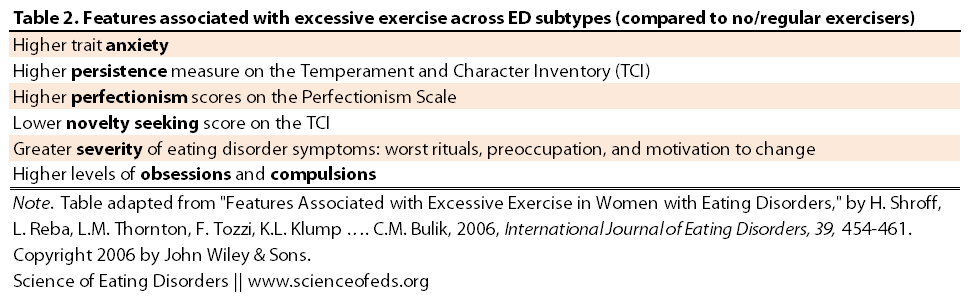
EE was associated with high scores on anxiety measures, persistence, and perfectionism and lower scores on novelty seeking. Excessive exercise was also associated with increased eating disorder severity (measured by evaluating rituals, food/weight preoccupation and motivation to change). This is not surprising (to me) because EE can be seen as way of self-harm, and so I’d hypothesize that patients who engage in EE probably exhibit worse ED psychopathology. Excessive exercisers also had higher levels of obsessions and compulsions.
SUMMARY
With regard to the finding that EE was most prevalent among the purging-type anorexia nervosa subgroup, the authors noted “previous research showing that this subgroup is particularly prone to anxious and harm avoidant traits.” Perhaps these traits somehow “feed into” excessive exercise or maybe exercise is a way to cope with the anxiety?
In a study with adolescent patients with AN, Davis et al. found that, compared with controls, patients reported engaging in more exercise during the year before the onset of their illness. Thus, it may be that individuals who are particularly prone to anxious obsessionality are more likely to engage in ‘‘extra’’ eating disorder behaviors (e.g., purging and excessive exercise) that are driven by their fear, anxiety, and obsessive preoccupation with weight gain.
An alternative explanation may be that exercise served to reduce or manage anxiety as postulated by Holtkamp et al. or to counteract prominent eating and weight related obsessions.
The authors hypothesized that the genes or neural pathways that predispose individuals to anxiety and excessive exercise may be linked. Or perhaps for this subset of individuals, exercise is just the most biologically sensical way to decrease anxiety:
Favaro et al. found significantly higher tryptophan to large, neutral amino acids (TRP-to-LNAA) ratios among those who exercised excessively. These investigators postulated that exercise helped to counteract the reduction of TRP/LNAA and serotonin synthesis, potentially functioning as a form of ‘‘self medication’’ to balance the levels of TRP/LNAA in the body.
These findings suggest that physical activity and weight regulation may, in fact, represent endophenotypes [what’s an endophenotype?] for eating pathology that contribute to its etiology, particularly the etiology of eating disorders characterized by high perfectionism, anxiety, ritualistic behaviors, obsessiveness, and purging behaviors.
From a clinical standpoint, EE seems to be associated with a number of features that might make treatment more difficult, such as increased eating disorder severity and lower BMI values. Understanding what drives EE in eating disordered individuals and who is predisposed to develop EE might aid in designing successful treatment interventions in the future.
Though keep in mind, this study was published 7 years ago–yes, “latest” is a flexible term around these parts–and I haven’t done a thorough search of what’s been published since, except I checked out the papers that cited this one.
However, there was a paper published in 2012 that suggested over-exercise is associated with suicidality in individuals with disordered eating (I plan to blog about this in the future). So there’s even more reason to study EE and its relationship with eating disorders in terms of causes, associations, and possible treatments.
I should also make it clear that in my mind, excessive exercise has got almost nothing to do with how much you exercise but your attitude toward exercise. My attitude toward exercise was at its worst when I was probably running only 25km/week, but if I missed a day, I’d panic, cry, and experience debilitating anxiety. I also wouldn’t listen to my body. Many years later, when I was training for the full marathon, I was running 70-80km a week and biking another 100-150km. I had no anxiety at ALL when I didn’t exercise, took days off when I felt I needed them, and carefully made sure I had no injuries, trained safely, and ate to fuel my runs.
Readers, have you ever exercised excessively (according to the definition in this paper, or in other papers)? During what stage of your eating disorder was the exercise at its worst? Do you have a sense of why you did it or why you were compelled to do it?
References
Shroff, H., Reba, L., Thornton, L., Tozzi, F., Klump, K., Berrettini, W., Brandt, H., Crawford, S., Crow, S., Fichter, M., Goldman, D., Halmi, K., Johnson, C., Kaplan, A., Keel, P., LaVia, M., Mitchell, J., Rotondo, A., Strober, M., Treasure, J., Blake Woodside, D., Kaye, W., & Bulik, C. (2006). Features associated with excessive exercise in women with eating disorders International Journal of Eating Disorders, 39 (6), 454-461 DOI: 10.1002/eat.20247
I recently wrote a paper on Exercise addiction which is the first time, I’ve really thought about exercise and its connection to my ED but I have definitely struggled with this problem for many years. I admit, I still struggle with it on occasion. So long as I refrain from it I’m ok, but I haven’t yet found a happy medium, because the urges return after a certain amount of exercise. Though I still struggle, there’s not doubt that it was at it’s worst when I as at my worst with AN. I really don’t know where it came from because I don’t recall knowing anyone with an ED as an avid exerciser. I do remember miserably pushing myself to my limits and becoming frantic if I weren’t able to run that day; other ED behaviors were used more frequently on those days. Today, I believe it is almost entirely a stress relief; the urge comes most frequently when I’m under a great deal of stress or suddenly feel very overwhelmed.
This article was very interesting to me, as I did little research on Exercise and EDs because my research indicated that there are two types of E Addiction: Primary, and Secondary. Secondary occurs only when accompanied by an ED, and as my paper was on E Addiction and not EDs I focused most of my attention in general addiction/excessive/compulsive/etc exercise, although I can say that there is no concrete definition for those either. The terms are often used interchangeably but in and of themselves hold different values to different people.
Very interesting article. Thank you for posting it.
Hi Mika, thanks for your comment!
“I admit, I still struggle with it on occasion. So long as I refrain from it I’m ok, but I haven’t yet found a happy medium, because the urges return after a certain amount of exercise. Though I still struggle, there’s not doubt that it was at it’s worst when I as at my worst with AN.”
I definitely know people in similar situations–they just have to refrain from it, otherwise it can get pretty bad pretty fast. So you definitely not alone.
“Today, I believe it is almost entirely a stress relief; the urge comes most frequently when I’m under a great deal of stress or suddenly feel very overwhelmed.”
This seems to echo Cathy’s comments (see below). For me, bingeing/purging was the go-to ED behaviour when I feel suddenly really overwhelmed or acutely stressed. If I manage to prevent that, exercise is the next thing down that list.
That’s interesting about primary and secondary exercise addiction. I don’t know much about exercise addiction in and of itself. You write “The terms are often used interchangeably but in and of themselves hold different values to different people.” What do you mean “hold different values to different people”? I’m really interested in what you found about how exercise addiction differs in those with eating disorders and those without (or at least how it presents/what it means to the individuals without EDs)?
Thanks again,
Tetyana
You write “The terms are often used interchangeably but in and of themselves hold different values to different people.” What do you mean “hold different values to different people”?
Yup, that’s exactly what I mean. There is a more widely agreed upon definition in the works thanks to the DSM-V, but most studies that have been conducted have included their own criteria of the condition. Here are a few pieces of my paper in regards to those definition. As I mentioned, my focus was primary addiction because my paper was not meant to focus on EDs but I’ve included a couple pieces of what I did find, in relationship to EDs.
“Exercise dependence is most commonly considered by psychologists, to be a behavioral addiction, and as such, cannot begin to be universally defined until the 2013 release of the DSM-V, which will include the definition and criteria for behavioral addictions. Consequently, the term exercise dependence is commonly interchanged with, or described by, the terms: exercise addiction, excessive exercise, obligatory exercise, compulsive exercising, and abusive exercising (Gapin, Etnier, & Tucker, 2009; Hamer, & Karageorghis, 2007).”
“The most widely accepted definition of exercise dependence has been defined by De Coverley Veale, according to modified criteria of the DSM-IV for substance dependence (Friemuth, et al., 2009; Kerr, Lindner, & Blaydon, 2007; Terry, Szabo, & Griffiths, 2004). Veale defines the criteria for primary exercise dependence according to preoccupation with exercise, significant withdrawal symptoms, preoccupation with exercise leading to the impairment of interpersonal or occupational relationships, and preoccupation with exercise for reasons not accounted for by another mental disorder (Allegre et al., 2006; Cockerill & Riddington, 1996; Gapin et al., 2009; Terry et al., 2004).”
“Exercise dependence produces consequences similar to other behavioral addictions and in some cases consequences similar to substance addictions and eating disorders (Freimuth et al., 2011). It affects reproductive health, mood and cognition, bones, soft tissue, immune system, and social and occupational life (Allegre et al., 2006; Rinaldi, 2004; Terry et al., 2004). Excessive exercise can cause amenorrhea, the ceasing of menstruation for a minimum of three month that can lead to fertility issues in women (Rinaldi, 2004). Amenorrhea leaves women particularly prone to osteoporosis; however, men are also at risk. This increases their likelihood of stress fractures to the bones (Rinaldi, 2004). These consequences are exponentially more prevalent in those with secondary exercise dependence, as the co-occurring eating disorder leads to the same problems. According to Freimuth (2011), clinicians often think the eating disorder symptoms that overlap with those in exercise dependence are limited to women but studies done at universities, show these problems are also found in men.”
“When an eating disorder accompanies the criteria for primary exercise dependence, the exercise addiction is a product of the eating disorder, therefore, secondary exercise dependence can be diagnosed (Allegre et al., 2006; Hamer & Karageorghis, 2007).”
“According to Freimuth et al. (2011), as many as 39-48% of people suffering from an eating disorder, also suffer from secondary exercise dependence.”
I hope this helps answer your question. Sorry I don’t have much more information. If you want the actual references so you can explore on your own, just let me know.
This one is easy for me to answer. Compulsive exercise was the biggest component of my ED – where the latter was diagnosed as (longstanding) restricting AN.
My ED started off with excessive exercising. As a child I was a competitive athlete. I learnt to swim at a young age and swam competitively from age 6 to age 10. This meant getting up very early in a morning to train before school. At age 10, my PE teacher recognised that I had a talent for endurance running and encouraged me to join the district athletics institute. I moved from swimming training to middle distance training.
I had always been an anxious, obsessive and compulsive person with a long history of OCD (see why structured athletic training suited me?!), but my anxiety levels increased around puberty. This increased anxiety may have been hormonally related, but I was also raped by someone in a position of power. I was also very self-conscious and disgusted with the bodily changes of puberty. I never perceived these changes as ‘fatness’ (I was very lean and slightly underweight), but I HATED growing boobs, in part because I felt all men were looking at me and wanted to rape me.
I discovered that my fears ‘melted away’ when I was training and started to run outside of scheduled training sessions – because it made me feel better. I was exercising hard for about 3 hours each day and I lost weight. I then started to follow the diet that my parents were on; not because I wanted to lose weight, but because following a diet plan made me feel (‘in control’) of my anxiety. Within a couple of months I was desperately underweight – at age 11. I was diagnosed with AN shortly after my 12th birthday.
Thereafter, exercise became the focal point of my AN. I exercised in secret, even bunking off school to run around the streets. I had a HUGE URGE to exercise to feel calm. Exercise has always made me feel very calm. When I used to exercise vigorously I sort of dissociated from the real world. I felt as if I was in a trance during and after exercise. I CRAVED that feeling.
I did some research in my 20s for my PhD examining the effects of repeated vigorous exercise and energy deprivation of the ratio of free tryptophan/BCAAs and the potential to increase brain 5-HT synthesis… I can send you the paper if you’re interested, Tetyana.
So to address you questions:
1. “During what stage of your eating disorder was the exercise at its worst?”
Answer: throughout. I only restricted hugely if I couldn’t exercise. But this had little to do with weight control or body image.
2. “Do you have a sense of why you did it or why you were compelled to do it?”
Answer: because it totally calmed me. I could be panic stricken with anxiety, but once I had been exercising vigorously for about 20 mins, that anxiety had melted away.
It is amazing and to some extent, almost scary, how much exercise can do to our state of mind. I also felt exercise really helped with anxiety, but I never experienced panic attacks, so perhaps the effects of exercise for me weren’t so acute?
“This increased anxiety may have been hormonally related, but I was also raped by someone in a position of power. I was also very self-conscious and disgusted with the bodily changes of puberty. I never perceived these changes as ‘fatness’ (I was very lean and slightly underweight), but I HATED growing boobs, in part because I felt all men were looking at me and wanted to rape me.”
I am really sorry to hear about the rate :(. I have never been sexually abused/assaulted, but I felt very much the same way. Losing my feminine figure was a nice side-effect of restriction. I really hated then, and I still really don’t like, sexual attention from the opposite-sex. I wouldn’t say my AN was centred around that, but it was a nice side-effect, and I can *definitely* see that for someone in your position, with your experiences, that would play a more dominant role.
I think I found the paper, from 1997?
Thanks, Tetyana 🙂
I viewed a reversal of the bodily effects of early puberty as a relief, yet my weight loss was unintentional. I recall Arthur Crisps theories of the 1970s and although I could identify with these, to some extent, I had never actually tried to lose weight. But once I had lost the weight I was fearful of seeing the number on the scales rise, even though I saw myself as too thin. As I have got older, I have lost the fear of weight gain, or looking sexual, but I do still have a dislike of the feeling of food inside me and exercise quite rigidly (though not excessively or intensely) to regulate my mood.
It had been so difficult trying to understand my ED and other behaviours, especially as running in the background is OCD in various guises.
Yes, the paper is 1997 and I did the research in 1995.
I have another paper that I will send you I would be interested in your viewpoint, given the discussions we’ve had recently. It’s autoethnographic and I had it published in 2009.
“I had never actually tried to lose weight. But once I had lost the weight I was fearful of seeing the number on the scales rise, even though I saw myself as too thin.”
This is how my eating disorder started, in a nutshell. I never set out to lose weight, at all, I just started eating healthier (and I used to eat JUNK all the time, like cake for lunch. I’m not kidding, I had disposable income because I started working in grade 8, so I bought a lot of unhealthy food.) And then once I lost weight, I became scared to see my weight increase even though I didn’t want to keep losing weight either (but I kept losing because I couldn’t eat more, or, when I ate, the guilt and anxiety was overwhelming). I wished I could just undereat and remain a normal weight. This was a common desire through-out my eating disorder history. Of course, most people assume the reverse, that many individuals just wish they could eat anything and be thin, I wanted the opposite (not always, but definitely many times). There were many times I wanted to be very thin, too. How I felt about eating, food, and weight weren’t particularly stable for me. Of course, neither was my eating disorder.
Yes, it takes years to publish anything, haha, I’m well aware of that :).
I have the other paper you are talking about, I just haven’t gotten around to reading it yet.
High degree of exercising is going to increase the expression of mitochondrial citrate synthase enzyme. This coincides with up-regulated genes fostering extra mitochondrial bio-genesis.
AN starvation leaves the body pressed to provide sufficient ATP.
Starvation limits the number of mitochondria from increasing & body holds off removing old mitochondria, even if key proteins damaged.
The EE boosted number of mitochondria provide more real time ATP. The exercise raises maximum oxygen uptake.
(Often hyper-activity precedes overt AN. The implication, to me, is sometimes pre-AN involves mitochondrial uncoupling protein dysfunction.)
Excessive exercise can raise the resting energy usage about 2.5 times above normal. It helps stay warm(thermo-genesis)in AN.
An experiment with 20% below weight rats given warmth resulted in them decreasing their excessive energy loss. And, furthermore, those warmed AN proxy rats went on to gain weight toward normal.
(I only see visitors to the tropics, not natives, with AN.)
Thank you for your comment Gringojay,
I don’t know too much about cellular metabolism except for what I learned in Biochemistry, but that was a long time ago. Exercise does a lot of things, including enhancing adult hippocampal neurogensis (I forget if the consensus is that it enhances neurogenesis or decreasing the rate of the massive apoptosis (cell death) that these new born cells go through. Perhaps this is my neuroscience bias, but I would tend to think that the effects of exercise on the neuronal activity and neuronal signalling probably play a bigger role in EE in eating disorders, compared to the effects of EE on cellular metabolism. Of course, everything is linked, but while this: “pre-AN involves mitochondrial uncoupling protein dysfunction” is interesting, I’m not sure, if true, how big of a role it would play in the etiology of the disorder and the EE component.
Having said that, I really don’t have a good background in cellular metabolism and it is role in neuropsychiatric disorders.
Thanks again for your comment.
Tropical natives do not need to regularly perform thermo-genesis. Most of the year they need to shed body heat.
Tropical natives are very prone to feel cold in their colder season. Visitors feel it like a delightful spring temperature.
Back in time humanoids were adapted to thrive in a hot environment. Looking at AN psychology as being the driver of brain physiology overlooks how relatively new some brain developments are.
The tropical native’s diet is very carbohydrate (tubers, breadfruit) based & lower in protein/fats. They are shunting carbon molecule’s of (blood sugar’s glucose derivatives through their mitochondria’s.
By using carbohydrate carbon intermediates for ATP they generate reactive oxygen species (ROS). But for them the ROS of H202 (hydrogen peroxide) is denatured into CO2 & H20 (water). It is this water that lets them carry heat out – natives didn’t evolve carrying water when away from a stream.
Starvation restriction of calories lifts the inhibition from SIRT 4(silent information regulator) in the mitochondria. This ends SIRT4 holding down expression of the enzyme glutamate dehydrogenase.
AN are running on that enzyme’s activity changing glutamate into alpha-ketoglutarate. They break down their own body protein into amino acids, like glutamate, for feeding into mitochondrial ATP assembly.
Protein based diets up-regulate uncoupling protein in the mitochondrial process. Uncoupling is what lets the carbon being processed produce heat (thermo-genesis) rather than ATP downstream. EE breaks free body protein & AN primitive neurology registers it has achieved better heat for ongoing life.
AN are low in leptin, & administering them leptin raises thermo-genesis. Only theraputic drawback is that leptin makes them
lose even more weight.
Hexo-kinase enzyme pathway, when blood sugar glucose is made into form body can work with, controls the leptin level. Lots of hexo-kinase enzyme activity = more leptin & conversely sparse hexo-kinase enzyme = less leptin.
The AN must switch to protein for it’s thermo-genesis – or reboot leptin output higher. The scarcity of AN in toasty tropical natives indicates genetic derailment happens with age in the AN regarding how it fuels itself (I suggest).
EE boosts the enzyme citrate synthase. The pre-AN is using the fatty acids they have at this pre-AN stage & putting fat’s carbon through beta-oxidation. It may be a compensation for epigenetic inhibition limiting glucose processing.
Which bring up the issue of how the pre-starvation AN’s glucose
they can’t put as carbon intermediates through their mitochondria affects their brain. (Elevating glucose inside a cell that doesn’t “burn” if for fuel alters transcription of genes in that cell’s nucleus. This is not a psychological problem, but it may alter self-perception so AN registers body image incorrectly; sort of how a dyslectic brain sees,
but actually mind percieves letters in reverse.)
EE for pre-AN with fat downstream yields the intermediary oxalo-acetate. With citrate synthase the oxaloacetate becomes citrate.
The citrate then converted into succinate & succinate is shunted into the mitochondria as an intermediary carbon leading to that carbon (originally pre-AN fat) being “burned” for ATP.
Why? Because the hexo-kinase pathway isn’t letting blood glucose be processed into citrate for running the “Citrate” cycle (now called the TCA cycle).
What happens to the pre-starved AN’s blood glucose? It is made into fat molecules. If not, then leptin would not be so low in AN. Once classic AN calorie restriction underway they don’t have much blood glucose to make into fat molecules. When pre-AN becomes full AN their lack of fat makes them fall back on protein.
(Protein is uncoupling-> heat -> cell sustains functional temperature.)
Thank you for your detailed comment.
“Looking at AN psychology as being the driver of brain physiology overlooks how relatively new some brain developments are.” How? I disagree with this. New is a relative term.
Also, do you have sources for the prevalence and incidence of AN in tropical countries? “The scarcity of AN in toasty tropical natives indicates genetic derailment happens with age in the AN regarding how it fuels itself (I suggest).”
So, are you suggesting that AN or EE in AN is predominantly driven by cellular metabolism? I am somewhat lost in terms of the “big picture” here, I must admit.
Tetyana
Yes, “new” brain a relative term.
~40 years in tropics & the natives with anorexia seemed due to parasites, not ANerviosa.
Modern ladies in urban tropics with AN seem media copy cats. They get studied (ex: Singapore, Jamaica), but no one is bothering to look for ANerviosa among the Kitavans.
My comments are certainly not covering the only AN factor. If
useful here’s about raising temps.
International Journal of Eating Disorders: Volume 45, Issue 1, pages 26–35, January 2012
“Warming … reversed running activity, preserved food-intake, and enabled female rats to recover from acute weight loss… indicative of the robust effect of AT (ambient temp.) in recovering rats from ABA(activity based anorexia).”
Volume 45, Issue 1, pages 26–35, January 2012
Hey Gringojay
I am really interested in learning more about all this, do you have any suggestions of good sources that I can read more about the ATP stuff?
Completely agree with your assertion that excessive exercise has everything to do with one’s attitude toward exercise, rather than the number of minutes or miles that comprise the workout. This, I think, is the problem with trying to quantify the “cut off” point for EE in terms of minutes/hours that I’ve seen done in some articles. Also, when I’ve heard EE discussed in more mainstream sources purporting to “raise awareness” about EE, it is discussed almost exclusively in terms of how much time an individual spent in the gym, etc. Not only is this problematic because you can’t really tell much about an individual’s approach to exercise by simply measuring the amount of time spent exercising, but sharing the message that “3 hours” or whatever amount of time constitutes EE automatically implies that less than that doesn’t. This is dangerous, in my mind, as individuals exhibiting severely problematic thoughts/actions/anxieties/fears related to exercise who don’t fit that description may feel that they don’t have a legitimate dependency on exercise. Yet another way in which the way we talk about eating disorders and associated behaviours creates categories of “in” and “out” that might compromise individuals’ ability to seek and obtain help and support…
Further, I wonder about the messaging surrounding exercise on shows like “The Biggest Loser” and how in a way, these shows normalize excessive exercise (for certain populations). How might these messages (ie. that one needs to abuse their “fat,” “lazy” body at the expense of mental wellness) play into delegitimizing the experiences of people presenting with anorexia or bulimia-like symptoms without an extremely low body weight? At weight does it become “not ok” to engage in such extreme exercise behaviours? Oh it’s a bag of worms…
Anyway, thanks for this post.
THIS. Seriously, I completely agree.
I always used to get very annoyed when people would tell me I was over-exercising when I was marathon-training and commuting by bike all around Toronto. I wasn’t, because my attitude toward it was very good. I was very flexible with my running schedule, shift my runs to fit social events and take days off when I felt I needed them. I also worked up to that level and I’ve never had any serious running or exercise-related injuries. But to non-exercising people, doing a 36km Sunday run was over-exercise. They didn’t get that I felt SO MUCH more anxious about exercise when I was in high-school and ran 3-5km/day, but my day would be RUINED, utterly ruined if I didn’t run at the right time (!!) even. I’d get anxious if I left the house at 7:10am, and not 7am. Whereas when I trained for my marathon (and other half-marathons I’ve done), I was completely flexible.
“This is dangerous, in my mind, as individuals exhibiting severely problematic thoughts/actions/anxieties/fears related to exercise who don’t fit that description may feel that they don’t have a legitimate dependency on exercise. Yet another way in which the way we talk about eating disorders and associated behaviours creates categories of “in” and “out” that might compromise individuals’ ability to seek and obtain help and support…”
YES. 100 times YES.
I also completely agree with you about The Biggest Loser thing. I have never watched it, but I have an idea about the show and what it is about. Somehow excessive exercise to the point of injury and complete exhaustion is *okay* when you are overweight?! No, sorry, it doesn’t work that way.
I have a history of AN-purging. This pretty much aligns with my feelings about it. I’ve only added the exercise component recently in the disorder. It is sorta double-edged. It reduces anxiety and feelings of needing to purge. But, this is probably because the exercise is serving a similar purpose to the purging. I’ve been trying to find a middle area, but I have difficulty discerning “normality” in regards to most things the disorder affects (food, weight, etc.) It also might really affect populations that tend toward OCD and perfectionism because exercise is a very logical process. I restrict food, count calories, count burned calories, look up workout plans, etc. It is a very plannable thing, which I obviously love. I am obsessed with anything involving lists, routines, and numbers.
You raise a really good point about planning that I really didn’t connect in this sense before. I always really loved calorie counting, it was negative/associated with an ED for only a brief period of time, when I was obsessed with eating under a certain amount, but during recovery I still counted (though mostly to make sure I was eating enough, and also because it was interesting, from a scientific perspective, to track how my weight changed with calorie intake, or how my calorie intake changed based on what was doing on in life).
When I used to do a lot of long-distance running, I also kept track of everything, again, not for an ED (I would stop running when my weight got low because I didn’t want to make it worse, I ate to run), but because it would help me avoid injuries, etc. I absolutely love keeping lists, a track of numbers, and having routines.
I don’t think I’ve connected how exercise fits into being such a “plannable” thing, as you say, so very true and I’m surprised I haven’t thought about that aspect of it. I linked it more to its anxiolytic effects.
It also makes sense because during periods of bulimia, for me, nothing was planned. It was utter chaos. Food, weight, everything in life.
I agree with it being a double-edged sword. I often found myself trying to remedy one component of the ED with another :/
Thanks for your comment Lauren!
I have exercised excessively and still do. For the last eight or so years of my life, I’ve been playing tennis for at least four hours a day (aside from when I spent three months out with a stress-fractured second metatarsal—during that time, I rode my bike for equally excessive periods of time). That said, anorexia in my case had exactly one phase, and I just described about half my life in mere sentences.
I’m not sure if it’s a compulsion anymore so much as an addiction. My depression kicks into high gear if I’ve gone even 8 hours (overnight) without exercise. The hilarious part is that my father tells me I’m “endorphin deficient” when I get depressed and then encourages me to exercise. I’ve convinced him it works better than either prozac or zoloft augmented with abilify (my current anti-depressent regimen) 🙂
It didn’t start that way though. My family has a gym membership, and my dad has an “I love saving money” membership. I figured that every minute I didn’t spend at the gym was money wasted, so I might as well fight atrophy of the wallet and the body. I feel like frugality with money and food sometimes go hand in hand.
I know this post is old but I want to comment on Leah’s comment about frugality with money and food because I think there is some weird connection between food/money/exercise for me that goes something like this:
1) My ED insists I don’t need food, or at least not very much
2) My financial issues convince me that not eating will save me tons on groceries
3) My OCD compels me to keep metrics and track all sorts of random things, including money and food and exercise, so I can plan out exactly how much I’m ‘saving’ in calories/dollars, along with how much I’ve ‘earned’ in exercise.
I also grew up in poverty so I wonder what factor that has in my attitudes towards food/money. I don’t mean to conflate EDs with food insecurity, because people with food insecurity due to macroeconomic/geographic/political/whatever factors are obviously a different population from anorexics with food availability, but I wonder if you’ve seen any studies that focus on those connections?
Interesting that you say that Eva, because lately I’ve recently come to similar conclusions. I completely understand the financial difficulties my be contributing to ED’s distorted thoughts. I’ve certainly seen that played out in my life…I’m glad you mentioned growing up in poverty and it’s possible contributions. I agree that “people with food insecurity due to macroeconomic/geographic/political/whatever factors are obviously a different population from anorexics with food availability.” Recently my PTSD has brought about flashbacks from when I was much younger and the way my mother specifically divided the food portions to ensure that each of us got at least a little food and thought to myself that same question. I don’t believe by any means that that was the reason for my ED but I’m sure having already been predisposed and the OCD and perfectionism having started at a young age that like the financial issues, the ‘rules’ around food as a child have also ‘supported’ ED’s distorted beliefs. I too would be interested in knowing if there have been any studies on the issue.