Many–myself included–assume that emphasizing the biological basis of mental disorders will reduce mental health stigma. The idea is that it will place less blame and personal responsibility on the affected individual.
Still, when it comes to raising awareness and reducing stigma, we need to make sure that our assumptions hold up to the evidence, otherwise we run the risk of playing a game of broken telephone. Given that this is Eating Disorder Awareness Week in the United States, the topic is particularly timely. Those of us involved in some aspect of mental health awareness don’t want to be saying “x” only to have be interpreted as “y.”
So, the question is–does a biological or genetic framing of eating disorders lead individuals to hold more positive views of eating disorder sufferers and place less blame on “weak will”?
This is precisely what Matthias Angermeyer and colleagues asked almost 1,350 individuals from two German cities. Angermeyer had them read two vignettes about a woman with either anorexia nervosa or bulimia nervosa (see below) and answer a series of questions aimed at probing the participants’ views on causal factors of EDs and their reactions toward ED sufferers.
The vignettes were:
Anorexia nervosa
In the last weeks 15-year-old Anna has lost a lot of weight with a strict diet and lots of sports. Her parents’ attempts to persuade her to eat are rejected vehemently by Anna. She herself has the feeling that she is overweight, even though she is significantly underweight in the meantime. Additionally, she is very afraid of putting on weight again.
Bulimia nervosa
15-year-old Bianca is very unhappy with her physique, even though her body weight is normal. She diets all the time because she wants to lose weight at all costs. Several times a week she experiences sudden cravings for food, then she eats big amounts of food in a short time. After that Bianca secretly vomits by putting a finger down her throat.
I cringed at the vignettes, but, I’ll put my criticisms on hold for a second and present what the researchers found (* = % that responded “somewhat true” and “completely true” and ** = % that responded “somewhat untrue” and “not true at all”):
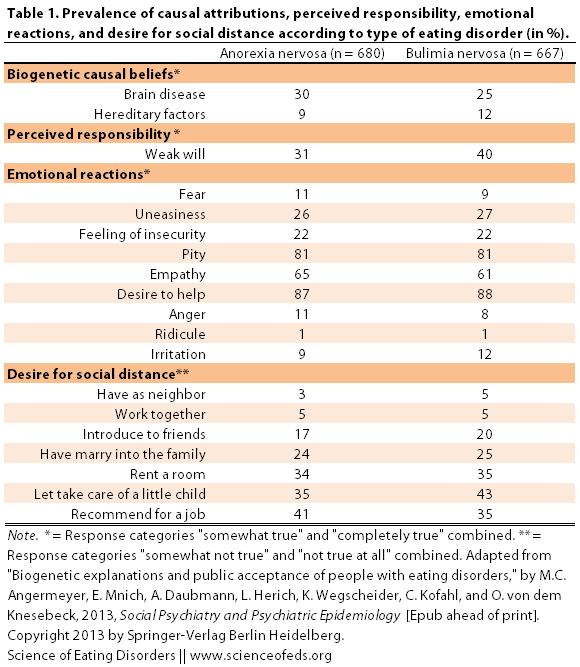
As you can see, there were few differences between attitudes toward anorexia nervosa and bulimia nervosa patients. What’s interesting, however, is that when Angermeyer and colleagues analysed the data further, the found that for both anorexia and bulimia nervosa, attribution to “brain disease” was positively associated with attribution to weak will. In other words, those that endorsed the “brain disease” as a causal explanation for EDs also held that individuals were more responsible for their condition.
This is both surprising and not at the same time. It is not surprising because this seems to be the case for other mental disorders, namely schizophrenia and depression. Studies have found that attribution to biological and genetic wasn’t particularly beneficial. On the other hand, it is surprising because unlike schizophrenia (though I don’t know about depression), eating disorder sufferers are not perceived as being dangerous and “crazy,” usually just vain, selfish, narcissistic and immature. In which cause, attributing the ED to biological causes should (as we commonly assume) give it more legitimacy, as opposed to make it seem “hard-wired”? (I think, anyway.)
The authors were at a loss for explanations, but they speculated:
Instead of conceiving brain disease and weak will to be in a reciprocal relationship, as proposed by attribution theory, in the sense that a stronger endorsement of the first is accompanied by a weaker endorsement of the latter, respondents may have perceived weak will as a consequence of rather than an alternative to brain disease, in the sense that people with this disorder are less able to exert control over their behavior.
Yeaaah this might be the case. I can think of some other reasons for these results, though.
First, the vignettes. Ugh, right? I mean, I get it, they are textbook/DSM-style blurbs. But they make Anna and Bianca look like vain, selfish, narcassitic and immature teenagers, don’t they? So much so that brain “disease” or not, their perceived psychological attributes still dominate our perception of them (at least this could be the case for many study participants). After all, what’s the point of presenting a very symptom-based and superficial description and then studying the effects of attributing EDs to biogenetic factors?
If I were to do the study, I’d do it differently. I would write up several different blurbs, each of which would have varying hints of biological and hereditary causal factors (mentioning anxiety, perfectionism, OCPD, family history, that restricting was anxiety-reducing, etc..), then split up my participants and give each group one a different blurb to read. Then I would ask them about their opinions and attitudes. Basically, my question is: To what extent do the responses depend on the content and wording of vignettes themselves? I bet substantially.
Second, “brain disease”? Would responses be different if Angermeyer said “brain disorder” or “brain-based disorder”? When I think brain disease, I think neurodegenerative diseases, encephalitis, brain trauma. Medical problems where there is a clear disruption in normal processes, either a particular group of neurons are dying (as in neurodegenerative diseases) or brain region is physical damaged, for example. The causes might be purely environmental (accident) or genetic (Huntingdon’s disease), but there’s a clear disruption in brain function.
Eating disorders don’t fit that in my opinion. The way I view it is that factors that predispose individuals to develop eating disorders aren’t inherently negative, they can just become maladaptive as a result of environmental factors. The personality and temperamental traits that commonly occur in those with eating disorders (and other mental health disorders) seem to me to be on one end of the normal distribution as opposed being on a whole different spectrum entirely. I think maladaptive behaviours are different from purely physiological diseases whose causes do not depend on the social environment (at least not much).
Finally, we don’t really know what the participants in this study thought when they read “brain disease” or “hereditary factors.” As someone with a neuroscience degree, it is particularly difficult for me to gauge public understanding and perception of biological phenomena. It would be nice to see, in future studies, more exploration (using semi-structured interviews) of what participants think of when they hear “brain disease” or “hereditary factors”. What does it mean to them?
In any case, I firmly believe that–although it is difficult, and it doesn’t fit nicely into a headline–we HAVE to emphasize and explain the complex causal factors that lead to eating disorders (and that means explaining a lot of biology, too). We don’t know them all yet, but we know enough to begin to paint a complex picture for the public. It is tempting to cut corners and make slogans that fit onto T-shirts, but I doubt that will get us where we want to be.
References
Angermeyer, M., Mnich, E., Daubmann, A., Herich, L., Wegscheider, K., Kofahl, C., & Knesebeck, O. (2013). Biogenetic explanations and public acceptance of people with eating disorders Social Psychiatry and Psychiatric Epidemiology DOI: 10.1007/s00127-012-0648-9
Agreed. . .
1 question – I didn’t read the paper,but do we know if the 1/3 that identified “brain disorder” (also a term I hate) was the SAME 1/3 that identified “weak will”?
“Brain disease,” actually. I don’t know if it is just me, but “brain disease” bothers me a lot, but “brain disorder” is only mildly annoying. Um, from memory, I don’t think it was THE SAME, just, higher those who put “brain disease” were more likely to also say “weak will.”
But they were in general the same people?
I’m just wondering if a separate 1/3 may have picked brain disease vs. weak will which might also account for their results
Right, this is from the paper:
“Contrary to what one might have expected, the attribution to brain disease was positively associated with the attribution
to weak will, i.e., the more respondents endorsed this causal explanation the more they tended to hold the person responsible for her condition.”
‘factors that predispose individuals to develop eating disorders aren’t inherently negative, they can just become maladaptive as a result of environmental factors. The personality and temperamental traits that commonly occur in those with eating disorders (and other mental health disorders) seem to me to be on one end of the normal distribution as opposed to being on a whole different spectrum entirely.’
This this this! You just put into words something I’ve been trying to articulate in my mind for ages. Are you considering becoming a science writer as a career? I’ve been reading your work for a while and I honestly think the mental health research world and the public would really benefit from your input.
P.S. I agree – ‘brain disease’ really sets my teeth on edge, but ‘brain disorder’ is slightly more tolerable. (Though I still don’t think it’s a good enough term to be spread publicly…not that I have any alternative suggestions!).
Anyway thanks for all your great posts!
Thank you for your wonderful comment, J! I’m glad that something resonates with you.
I’d absolutely LOVE to have a career in science communication, but at what level and what exactly, I’m not sure. There’s great freedom in doing this as a hobby with no boss and no pressure to have this bring me income because it means that I can write whatever I want, which is nice.
I’d love to do something on the knowledge translation side of things (http://www.cihr-irsc.gc.ca/e/29418.html).
But thank you–that means a lot to me! I am super happy to know that this blog is helpful and interesting to others. It is really amazing, actually.
Yeah, I don’t know, why can’t we stick to mental disorder, you know? What’s wrong with that? (Thoughts? Maybe I’m missing something).
True…maybe you could do some freelance work, on top of a ‘steady’ job in knowledge translation. That way you’d get to keep your freedom/independence to write about what you want, while still having a dependable income from an equally enjoyable job. Wow I just decided your future for you – that was easy! hehe.
No but seriously, I am constantly frustrated because I’m ridiculously well-versed in ED research (I don’t mean that in an arrogant way – it’s not a good thing – long story involving AN, OCD, PhD, a couple of ED journal publications, having to leave uni, unemployment, obsessiveness and waaaay too much down time)…and as you know, the research is so commonly misreported, misinterpreted and oversimplified, even by other researchers or ‘experts’ in the field (well, in my opinion).
But I’m not in a position to be able to really articulate or communicate anything (thanks brain)so I just sit impotently fuming, haha. And you’re one of the first people I’ve seen to actually interpret and communicate research properly, with a real understanding of research methods and the impact of research design and flaws (which is so important), and you never jump to conclusions or fall back on easy cliches or propagate catchy slogans based on faulty interpretations of data.
So even though I’ve always already read the original articles you post about (remember when I said ‘ridiculously well-versed?’ ugh this is how lame I am), I always look forward to your posts because you see things a lot more clearly than I do and you articulate things I’ve been thinking but have trouble putting into words (my brain is just not coherent at the moment), and you always point out things I haven’t thought of (which, honestly, is a very refreshing experience for me – haha that sounds stuck-up but I’m really not meaning it to be).
Also, you have a far superior understanding of the neuro side of things and science in general (superior to me, and to most people, I imagine) which I think makes you extra valuable in this field. Not to mention it makes me so happy to see you combating what I see as unhelpful and misleading awareness campaigns, which, while well-intentioned, are often based on exaggerations and lack of understanding of statistics. Etc etc. So…seriously, thank you.
Well, now that I’ve probably convinced you that you have a crazy frustrated academic stalker on your hands…haha sorry if I got a little fervent there. And you can see what I mean by being inarticulate by the ramblingness of this comment! I don’t normally comment because I’m pretty paranoid about the internet but…yes…thought it was time to express my appreciation for your work 🙂
Officially shutting up now 😉
Holy crap! That’s one of the nicest things anyone has ever said to me! Thank you!!! It is just so amazing and satisfying to do what I REALLY like doing and have others enjoy it, too. Absolutely amazing. Thank you!!
And I love how you picked a career for me, haha. I think I’m going to stick to private tutoring and freelance editing and try to expand that for now. I love the flexibility and diversity of the work, and the fact that it gives me time to do this! 🙂
Tetyana
Interesting concept.. I never know how to explain my difficulties to people in a way that I feel will be acceptable to them. I do fear rejection as a consequence of my mental health difficulties.
Of course, I could say nothing whatsoever, but anyone who spends more than a small amount of time with me notices that I have difficulties. I can fake being ‘normal’ and OK for a short period of time only.
I have a long history of anorexia nervosa (AN), from which I am significantly recovered. Or maybe it would be more accurate to state that I ‘manage’ the AN. I eat well to maintain my weight, but sometimes I really struggle with food and the urge to over-exercise.
On top of that I have OCD and am socially anxious. I am very obsessive about routines and doing things a certain way. I have a number of autistic traits. It’s so damn wearing trying to appear ‘normal’ in company and not to freak out and have a panic attack because my routine changes, something unexpected happens, or I cannot wash my hands as regularly as I feel I need to.
I have talked to my psychiatrist about this a lot. I need a word that will encapsulate my difficulties that is acceptable to the majority. I need to be able to explain that I just cannot cope with certain things in life, without sounding ‘difficult’ or ‘self-absorbed’. The truth of the matter is that I really cannot cope at times. I don’t want to have meltdowns in public. I need to feel understood and accepted and I don’t know the bast way to do this.
Really interesting and really important discussion!
I think the crux of the ‘naming’ issue really lies in the fact that people don’t really ‘get’ (as in, understand) eating disorders, unless they’ve experienced one.
Personally, I have mixed feelings on the subject. I think it’s incredibly de-motivating to be told you have a ‘flawed brain’, and thus are (and perhaps always will be) sick– as you can’t ‘fix’ biology. At the same time, I think it’s just as demotivating to tell someone that the answer lies completely with their own present choices and behaviors. That dismisses the real fact that there are biological issues at play, and places undue ‘blame’ on the person with the ED.
On the other hand, I cannot even express the level of rage that wells up inside me when I hear someone’s psychosocial history (in the context of how it correlated with the initiation and/or continuation of their ED), and someone who may have played a role in that psychosocial history uses the ‘brain disorder’ argument to categorically and summarily deny that they may have made any possible action or comment that may have influenced that person in any possible negative way– ever. I think it’s far too convenient of an ‘escape’ button when friends/family/communities/etc want to dismiss a person’s actual feelings, history, experiences of trauma, lack of support, etc, etc, etc.
Ultimately, my vote lies with describing the illnesses as being biopsychosocial in context. This, to me, is the best way to really capture the fact that there are biological, sociological, and psychological factors that ALL play a role.
While separating the different aspects of the ED may be helpful at times (i.e. helping to ease the distress someone is feeling when they can’t just snap their fingers and ‘stop doing that’), the flip side is that these different aspects can also be used in order to *dismiss* the impact that another factor may have on the patient (and usually when it is most convenient to the person claiming an affinity to any particular causal factor).
Yeah, I generally agree, although I get so annoyed when people decide to label one phenotype as “flawed”… no, it is just the outcome of specific predispositions and environmental factors. It is not flawed, maladaptive, sure, but it is not a “flaw” in my opinion. And while we can’t change our DNA, epigenetics and neurobiology are not stable throughout life — clearly, because people get sick and get better, too. I think biopsychosocial or neuropsychiatric captures the essence better than “brain disorder.”
(I think some people can really understand EDs quite well without ever experiencing one, though I think that requires years, if not decades, of clinical practice or research, and even then, it is not always the case.)
One reason why weak will might grow may be specific to eating disorders. A study on perceptions of eating disorders found that ordinary people have many misconceptions. They regard eating disorders as a lifestyle choice. However, they see patients who have them as strong willed. Having it explained as a biological impulse might consequently diminish that.