Cholecystokinin (CCK) is a digestive hormone that stimulates fat and protein digestion, and promotes the feeling of satiety. CCK is released after food consumption to promote digestion (by releasing digestive enzymes from the pancreas and stimulating bile secretion). In rats and monkeys, injection of CCK induces satiety, though it seems (from what I’ve skimmed), the extent to which CCK regulates food intake in humans is not well-established. Previous research on the role of CCK in anorexia nervosa (AN) has found conflicting results, in part because of methodological issues related to measuring levels of CCK. In a recent study, Cuntz and colleagues (2013, freely available online), having developed a better assay for measuring CCK, wanted to clarify its role in AN patients.
The authors had the following goals and hypotheses (I omitted one):
- Objective 1: Compare CCK levels between AN patients and healthy controls before and after a meal
- Objective 2: Given the difficulties AN patients have in the initial stages of weight gain, the authors hypothesized that in the early stages of weight gain, AN patients would have higher levels of CCK and/or rates of CCK release after a meal than healthy controls, which would induce a premature feeling of satiety
- Objective 3: Compare CCK release in restricting (AN-R) versus binge/purge patients (AN-BP)
- Objective 4: Determine whether CCK release is related to gastrointestinal complaints in AN patients (based on the fact that CCK plays a role in GI disorders)
Participants were 23 AN patients (10 AN-R, 13 AN-BP) and 8 healthy controls. CCK levels were measured after a standardised test meal between 7 – 8 a.m. following a 12-hour fast. This test was performed on three different occasions:
- Time point 1: Within first few days of admission with no weight gain in the previous two weeks
- Time point 2: After an initial weight gain of at least 2 kg for two consecutive weigh-ins
- Time point 3: During last week before discharge after a minimal weight gain of 4 kg (8.8lbs)
SUMMAry OF MAIN FINDINGS
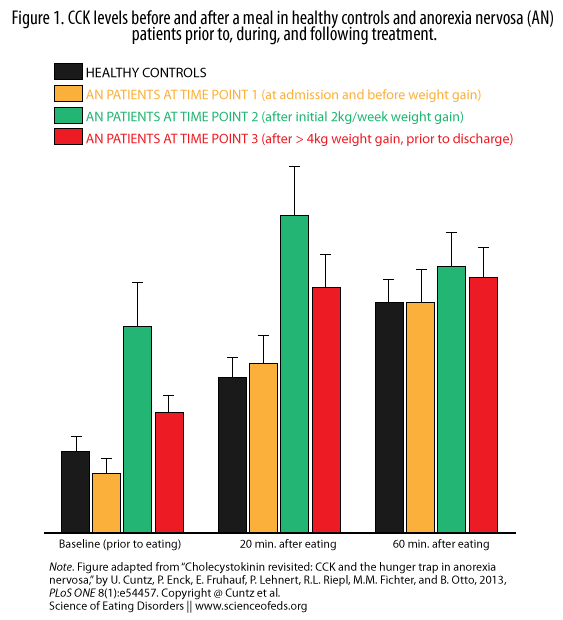
The main findings, illustrated in Figure 1 below (which I replicated from the paper and tried to make clearer), are as follows:
1. Objective 1: Prior to any weight gain (right after admission), levels of CCK before and following a meal were comparable between AN patients and healthy controls. This is evident in the figure below, where the first two bars in every set (black and yellow/orange) are similar before eating (baseline), 20 minutes after eating, and 60 minutes after eating.
What does this mean?
Essentially, it probably means that long-term/severe AN patients (regardless of subtype) become well adapted to chronic malnutrition and respond normally after a small meal.
What they found next is, I think, the most interesting part of the paper:
Objective 2: After initial weight gain, both baseline and post-meal (20 min) CCK levels increased dramatically compared to healthy controls . You can see this in the graph by comparing the green and black bars in the first two sets.
What does this mean and what are the implications?
According to common clinical experience, such a strong response to moderate food intake may be able to limit and counteract the therapeutic attempts to further gain weight. It may explain the increasing difficulties that anorexic patients perceive in the first weeks of weight gain to maintain a sufficient food intake. This phenomenon may be called a ‘‘hunger trap’’: Once the CCK system has adapted to low food intake, it self-limits weight gain by increasing satiety even with moderate food intake. Only with further weight gain the CCK release returns to the initial and normal state.
The good news: CCK levels, thought still higher than healthy controls, began to normalize after further weight gain (red bars). The researchers didn’t follow the subjects for long enough to see how much weight/time is required to return to the levels of healthy controls (and if that happens), but it is certainly promising.
Objective 3: There were small but consistent differences in CCK release between AN-R and AN-BP patients patients (not shown in Figure 1). Overall, AN-BP patients showed lower CCK levels at all time points. This makes sense and may explain why AN-BP patients are more prone to binge eat and “lose control.”
Objective 4: The authors found a moderate relationship between CCK levels and gastrointestinal complaints and subjective GI-related impairment at the first and second time points, but not at the last time point (not shown in Figure 1). The authors hypothesized that this may mean that the relationship between CCK and GI symptoms is strong in disordered eating/eating disorders but decreases once things begin to return to normal.
SO, WHAT DOES ALL OF THIS MEAN?
I’ll let the authors explain:
Anorexic patients, specifically of restricting-type AN show well adapted CCK-release pattern with stable but abnormal eating behavior and under-nutrition. With the initiation of weight gain, an initial exaggerated CCK-response occurs that – clinically – may terminate further weight gain by inducing premature satiety (‘‘hunger trap’’). Only if therapy can overcome this intrinsic handicap, further weight gain will lead to normalization of CCK levels again. Patients who do not adapt to the normalization of CCK are at risk to experience high levels of gastrointestinal symptoms that do not improve with weight therapy.
The authors did not provide any practical advice or information on what could be done to alleviate this exaggerated CCK response and/or the associated GI symptoms. However, information is power and knowing that this even happens (at least based on this study, we have to wait for it to be replicated) can make it easier for the patient, their family, and the medical team. The way I see it is that it might remove some of the blame or guilt on the part of the patient (for why eating more is hard) but also assure them that, more likely the not, CCK responses will normalize with continued weight gain, as will the associated GI symptoms.
References
Cuntz, U., Enck, P., Frühauf, E., Lehnert, P., Riepl, R.L., Fichter, M.M., & Otto, B. (2013). Cholecystokinin revisited: CCK and the hunger trap in anorexia nervosa. PloS ONE, 8 (1) PMID: 23349895
I think these data fit well with the literature on the “settling points” hypothesis of weight regulation. Regardless of whether a stabilized weight is over/under what is healthy, bodies tend to defend (+ or – about 5-10 lbs) their current state. Dramatic lifestyle changes must occur to effectively move the settling point to a newer, more healthy level. I see an emphasis of this more on the dieting side of things (i.e., as one of the explanations for why most conventional diets don’t work), but I have never heard discussions of this topic for AN.
Good point, yeah. And CCK is, then, just a small component of probably a much larger system trying to “defend” a certain state.
I am absolutely not knowledgeable in this though.
I think it would be interesting to see the levels of CCK in people without AN prior to and after 2 kg increase (although it would be highly unethical to pursue this kind of experimental condition on normal people!) to see whether the increase in CCK demonstrates a reflexive physiological change in all humans in response to weight gain.
That’s a really good point! I’m not sure if it would be unethical per se (you could always probably test it as part of a larger study for something else and then retest people who happened to gain weight for whatever reason). Unfortunately, I don’t know enough about this kind of stuff, it almost seems like something that surely must have been done before?