This study is a follow up on the previous study (last entry) which examined the problems with the EDNOS classification, the frequency of transitions between eating disorders and how the DSM should be changed to reflect the clinical reality of eating disorders (and what is the clinical reality?)
In this study, Eddy and colleagues followed 246 women who were initially diagnosed with either AN or BN, for an average of 9 years. The main goal was to study the growing disparity between (1) the consensus that eating disorders are not stable overtime and how (2) the current diagnostic criteria which do not adequately address this, by following the clinical presentation of EDs overtime and providing suggestions for the upcoming DSM-V.
EDNOS is an often ignored category in research–in main part because it is difficult to study such a heterogeneous group. Nonetheless, Eddy et al. summarize some interesting findings on diagnostic crossovers and subthreshold EDs:
- No substantial differences between full-blown and subthreshold (EDNOS) syndromes
- Majority of EDNOS patients have a history of a full-syndrome (82%, Herzog et al. 1993)
- EDNOS and diagnostic crossovers are common: In a 30 month study by Milos et al. (2005): 20% and 27% of AN and BN patients, respectively, crossed over to EDNOS; from the EDNOS category: 14% crossed to AN, 3.4% to BN and a slight majority to recovery
How does this present paper differ from the 2008 paper? It doesn’t differ a lot in the methods, but it expands the scope of the research study to include subthreshold/EDNOS periods and assess the psychosocial functioning of patients for the duration of the study. The question of interest is: is there a relationship between symptom presentation and psychosocial functioning?
First, what does subthreshold mean, in this study?
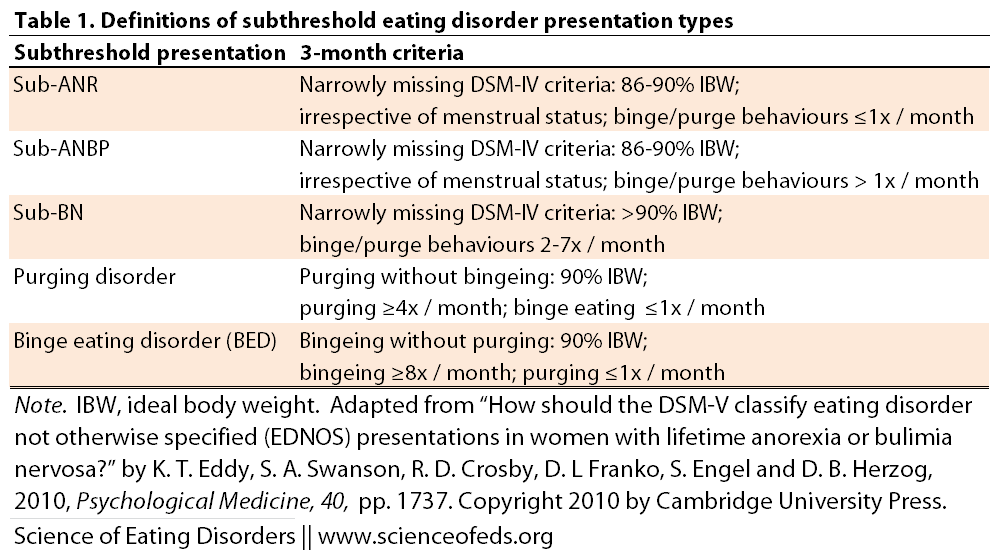
SUMMARY OF MAIN FINDINGS:
Transitions
- 77.6% of all patients developed subthreshold AN or BN for 3 month or more (the break down is: ANR (64.7%); ANBP (67.1%), and BN (91.8%)
- Individuals were more likely to develop subthreshold presentations of their initial diagnoses than a different diagnosis or to transition into recovery (45% likelihood to go from full-syndrome to subthreshold; 42% to a different full-syndrome and 13% to recovery)
- Once in the subthreshold category: 36% returned to full-syndromes and 41% to recovery (this is not a significant difference, meaning equal likelihood)
- Patients in subthreshold AN/BN were more likely to transition to recovery that during full-syndrome AN/BN; except for subthreshold ANBP, where there was <5% probability to proceed to recovery
Psychosocial
- ANR group experienced improved psychosocial functioning for all periods except during ANBP
- For women with ANBP or BN: all subthreshold presentations and recovery were associated with improved psychosocial functioning
- Interestingly, unlike all the other groups, there were no significant differences between subthreshold ANBP and recovery in the ANBP group
- In the BN group there was no difference between ANR and recovery
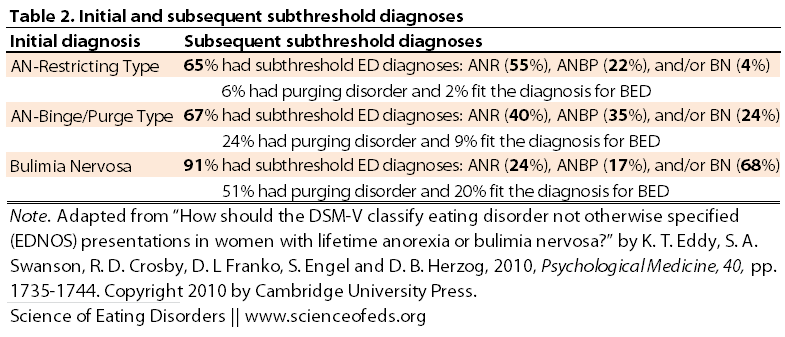
Summary of the findings based on initial diagnosis. A figure and table format illustrating the probability of transitioning to various subthreshold disorders, purging disorder and BED during recovery from anorexia and bulimia nervosa:
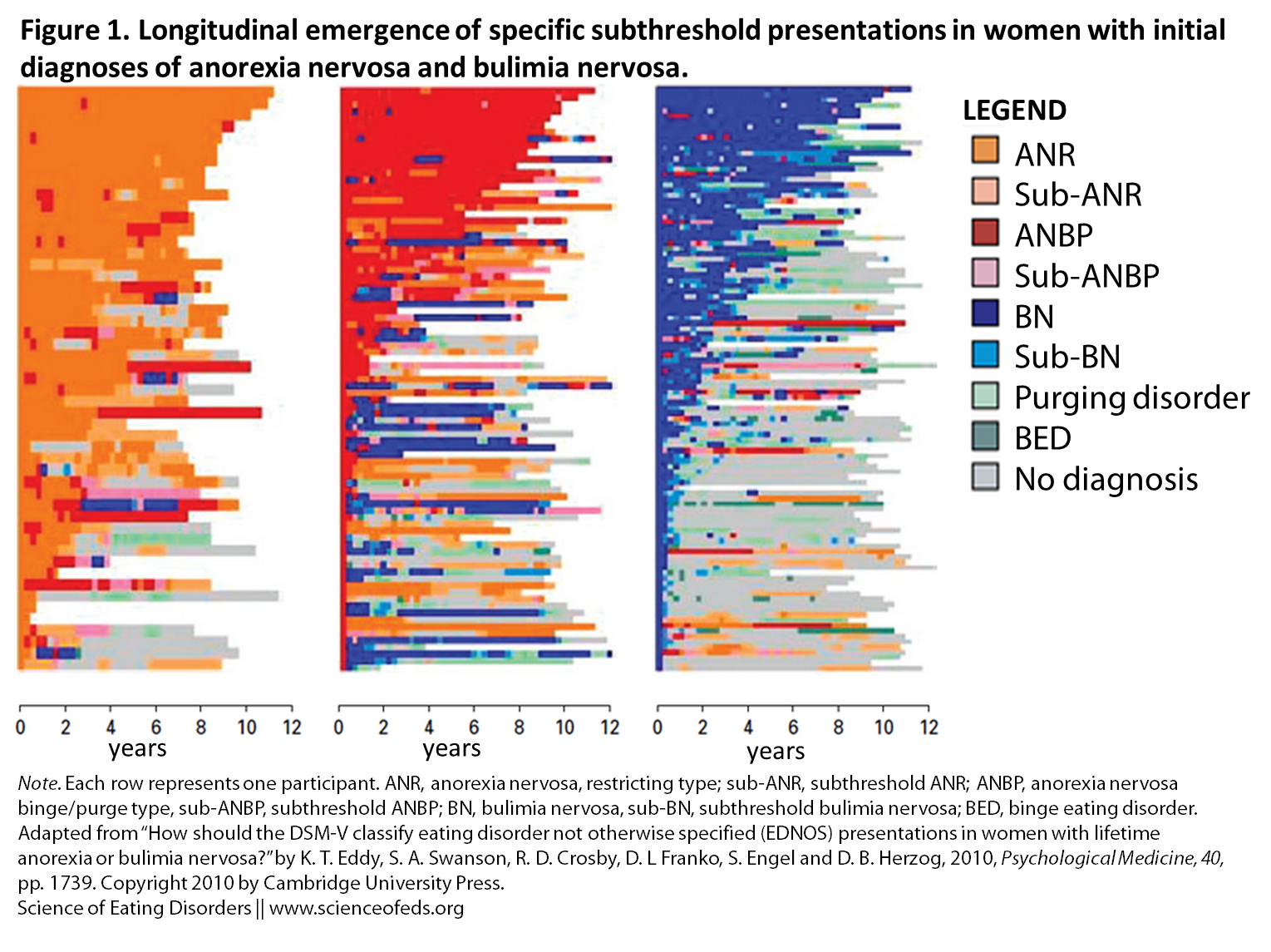
Here is a summary of the information in the above figure:
CONCLUDING THOUGHTS
EDNOS seems to be a stage that many patients go through on the way to partial or full-recovery as well as during transitions between full-syndromes. The duration of subthreshold EDs differs from a few month to many many years, reflecting, perhaps, that for some individuals, subthreshold EDs may be synonymous with partial recovery. I think that’s to be expected, given that EDNOS is defined as missing at least one criterion for a full-diagnosis. In AN that tends to be the weight or amenorrhea criteria, and in BN, the frequency of bingeing and purging behaviour.
But it is important to keep in mind that while EDNOS may often correlate, or indeed be synonymous with partial recovery, this is not always the case. Subthreshold AN or BN diagnoses may mistakenly be assumed to be less severe versions of a full-blown syndrome, and thus a less severe presentation of an eating disorder, but this need not be the case: an individual may binge/purge less than what’s required for a full BN diagnoses, not be low enough in weight for AN, but nonetheless, have infrequent but extreme bingeing and purging episodes and fast, abuse laxatives and diuretics for the other 6 days of the week.
Eddy et al. conclude with an important message for clinicians and the DSM-5 working group:
For the majority of individuals with lifetime AN and/or BN, the course of their illness will be marked by symptom fluctuations that could be clinically described as EDNOS… these data suggest these subthreshold presentations are a part of the course of illness.. rather than different disorders… Our data do not suggest that these subthreshold presentations in women with lifetime AN or BN are distinct enough from the AN or BN to warrant a separate diagnosis as they are similar in symptomatic presentation, often time-limited, and not directive of course/outcome. Importantly, these findings raise questions about when and if it is ever appropriate to diagnose EDNOS in individuals with lifetime AN or BN.
References
Eddy, K.T., Swanson, S.A., Crosby, R.D., Franko, D.L., Engel, S., & Herzog, D.B. (2010). How should DSM-V classify eating disorder not otherwise specified (EDNOS) presentations in women with lifetime anorexia or bulimia nervosa? Psychological Medicine, 40 (10), 1735-1744 PMID: 20047706
As someone who may (decisions decisions) be interested in doing eating disorder research someday in graduate school, I am VERY excited about this website! Looks great 🙂
Are you currently in undergrad? Let me know if there’s anything in particular you are interested in!
I’m not sure if this article makes me feel worse because it’s not overly optimistic, or if it makes me feel more normal and thus better for still struggling even though I no longer fit the criteria for the ED with which I was diagnosed. Either way, though, it was a good thing to read. Thank you.
I tend to feel that overall it is a good thing, because it supports the notion that ED’s can be a long-term, fluctuating, illness. Symptom remission doesn’t mean you are not prone to relapse. I also like that this study (and the one in my last post by the same group) make it pretty clear that someone that is EDNOS or “partially recovered” (what’s the difference anyway?) is still symptomatic and, frankly, likely to be in transition between diagnosable disorders (I know that’s been true for me). I think people tend to feel they are not as sick or don’t deserve treatment, or they failed at being sick (particularly true for anorexia, I think) if they don’t fit the full criteria, but I think that’s BS, it is a mental disorder first and foremost. Showing that EDNOS is really part of the same picture as AN and BN, I think, overall, is good for the field.
Interesting. I feel weird since I used to be “officially” bulimic for 7 years and now I’m EDNOS, I guess. I just keep saying “recovering from bulimia” despite not recovering. I just dont throw up anymore, most of the time.
This brings up the point that partial recovery = EDNOS for those who’ve fulfilled the full criteria for AN or BN. And EDNOS is really just sub-threshold ED, which can probably be classified into binge-purging type or non binge-purging type.
Do you think there’s a significant difference between how you felt mentally when you were “officially” bulimic and now? (You obviously don’t have to answer if you don’t feel comfortable).
Thanks for the reply.